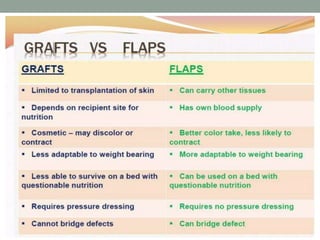
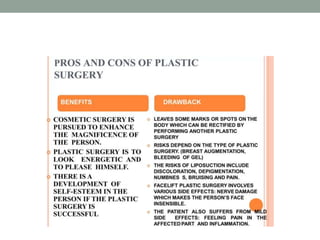
Plastic surgery, a medical specialty focused on restoring form and function, encompasses reconstructive and cosmetic procedures, often involving skin grafting. Reconstructive surgery aims to correct functional impairments from trauma or congenital defects, while cosmetic surgery focuses on enhancing aesthetic appearance. Key principles include minimizing scarring and ensuring proper healing, with careful post-operative care being crucial for successful outcomes.















![Reconstructive and cosmetic surgeries [Auto-saved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/reconstructiveandcosmeticsurgeriesauto-saved-230621074305-25a142e9-thumbnail.jpg?width=640&height=640&fit=bounds)











![Special dermalogiacl therapyies [final]](https://cdn.slidesharecdn.com/ss_thumbnails/specialdermalogiacltherapyiesfinal-200717060942-thumbnail.jpg?width=640&height=640&fit=bounds)





































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












