Download to read offline





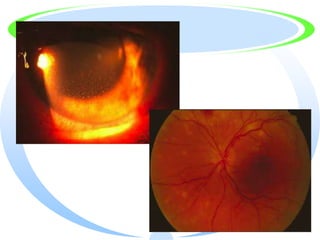
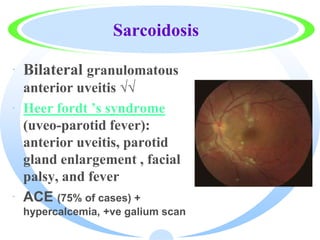




1) This document summarizes different types of uveitis including anterior uveitis, intermediate uveitis, and granulomatous anterior uveitis. It discusses various etiologies and presentations of each type. 2) Treatment recommendations are provided for each condition including topical and systemic medications as well as surgical interventions if needed. Conditions like tuberculosis, toxoplasmosis, sarcoidosis, Behcet's disease, and others are addressed. 3) The author argues that secularism does not answer existential questions about the meaning of life. While it promotes ideas of freedom and rationality, it does not provide spiritual guidance and can lead people to make wrong choices by thinking they have freedom





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














