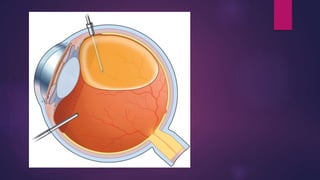
Silicon oil is commonly used in retinal detachment surgery to tamponade the retina. It is removed after sufficient chorioretinal adhesion has occurred, usually between 6 weeks to 6 months. Silicon oil removal requires careful active aspiration using two cannulas for infusion and suction to remove all oil from the eye. Residual oil droplets can cause floaters so multiple fluid-air exchanges are done at the end to remove any remaining oil. Complete removal is important to prevent further retinal detachment which occurs in around 10% of cases after silicon oil removal.