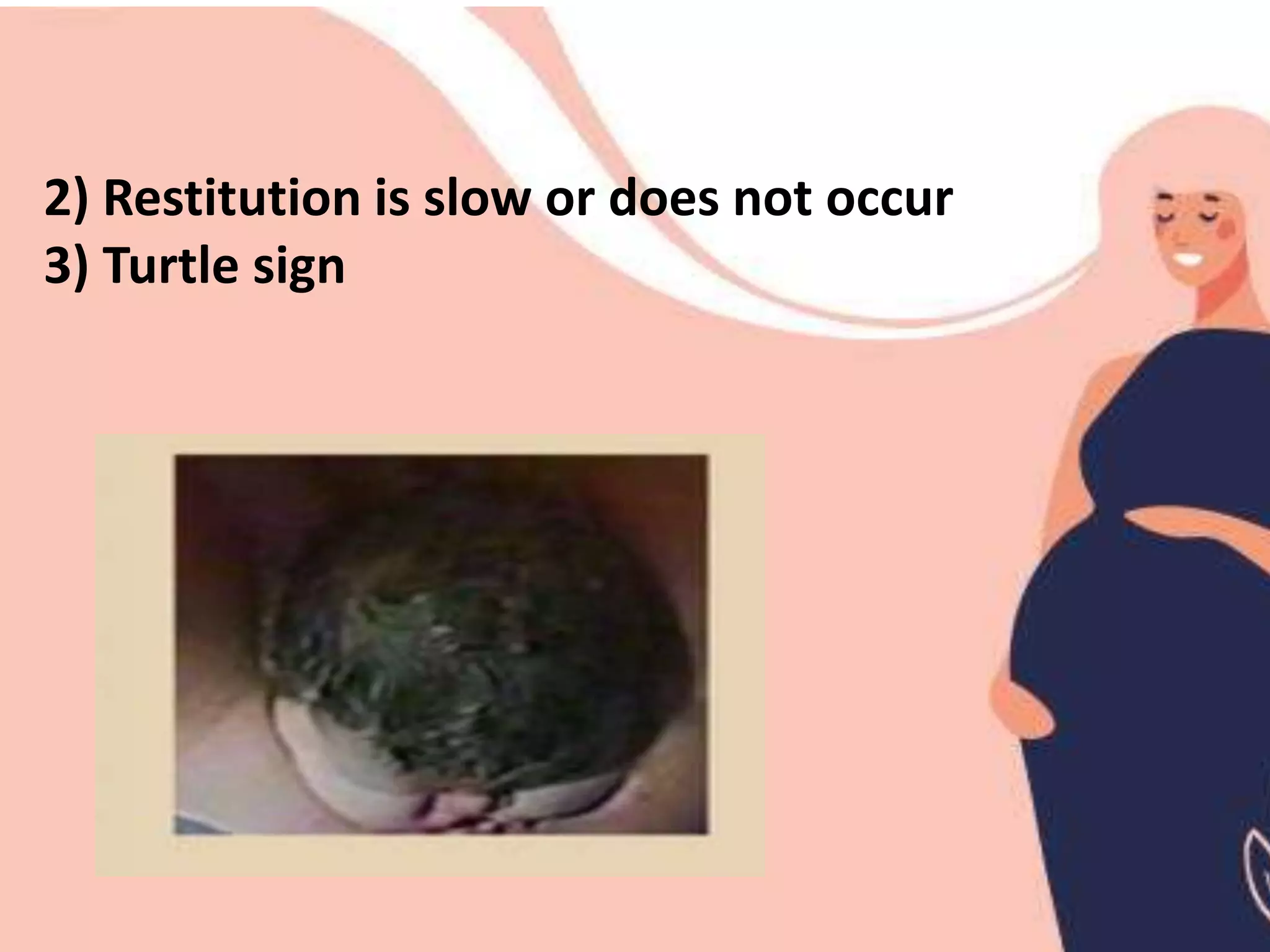
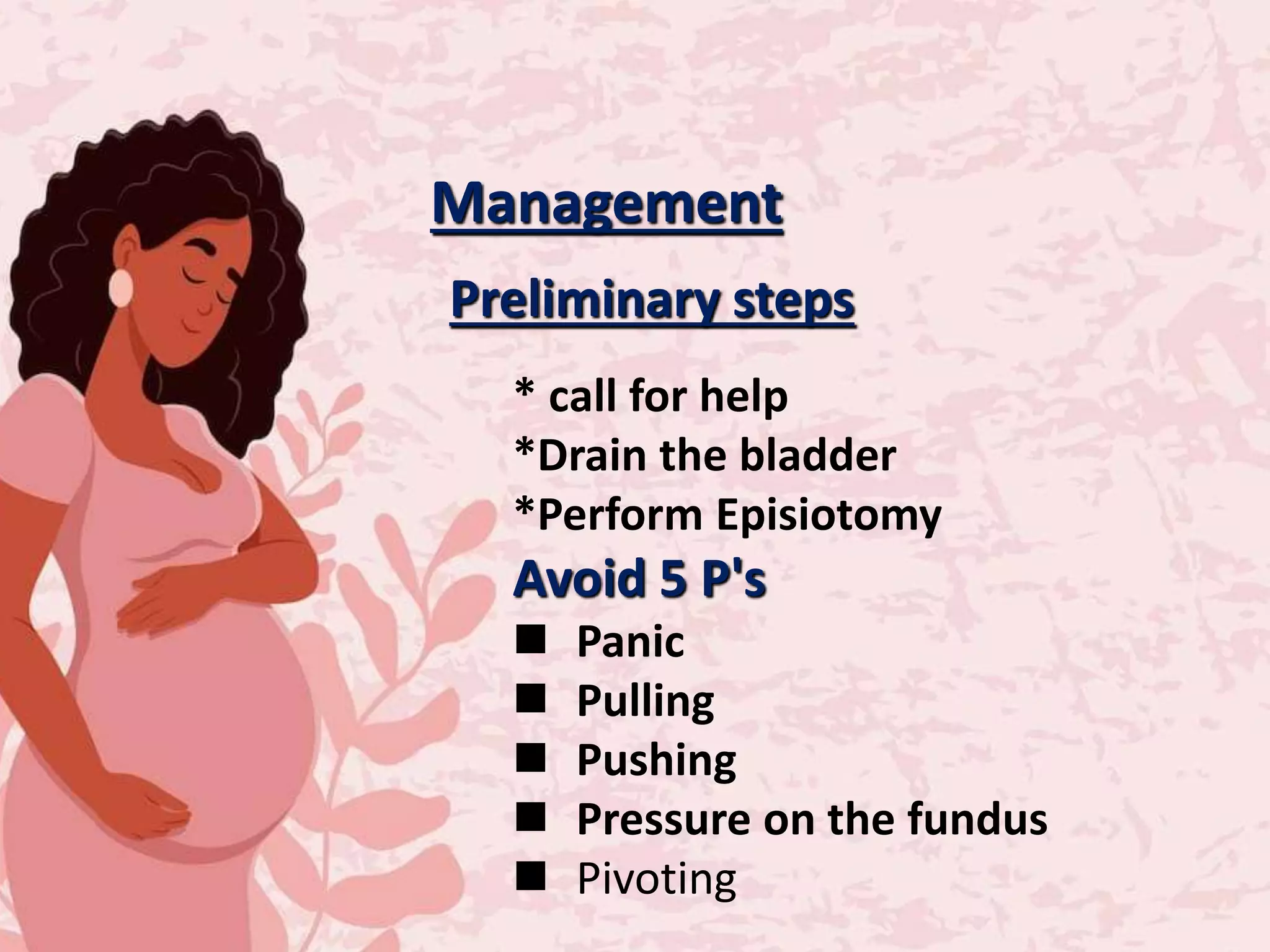
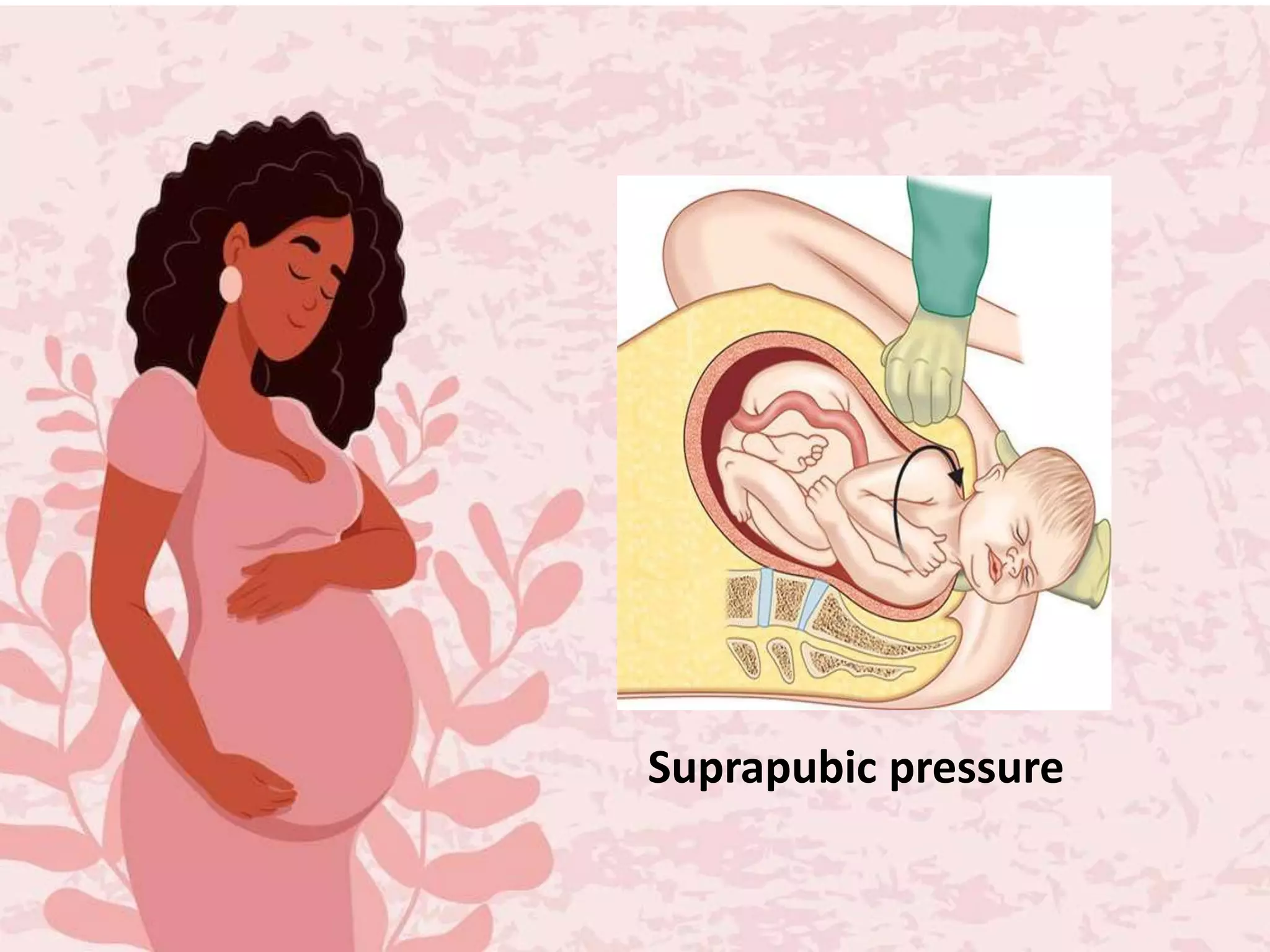
Shoulder dystocia is defined as when the fetal head delivers but the shoulders do not deliver spontaneously or with normal traction. It has an incidence of 0.6-1% and is caused by an increase in fetal size relative to the head. Risk factors include maternal diabetes, obesity, macrosomia, and a previous history of shoulder dystocia. Management involves preliminary steps like calling for help and draining the bladder, followed by maneuvers like McRoberts, suprapubic pressure, or rotating the posterior shoulder anteriorly. Complications can include newborn death, asphyxia, brachial plexus injury, or maternal hemorrhage.

































































![7-Shoulder_dystocia[1].pptx5555555555555555555555](https://cdn.slidesharecdn.com/ss_thumbnails/7-shoulderdystocia1-240901140722-b7a2771f-thumbnail.jpg?width=640&height=640&fit=bounds)


























