Downloaded 314 times












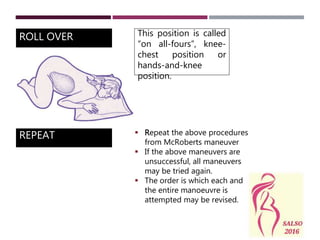




Shoulder dystocia is when the baby's anterior shoulder gets stuck behind the pubic bone after the head delivers. It can cause injuries and is a risk factor for litigation. The document outlines steps to diagnose, manage, and prevent complications of shoulder dystocia through early detection of risk signs, use of maneuvers like McRoberts position and suprapubic pressure, and documenting interventions taken. While risk factors exist, shoulder dystocia can occur unexpectedly so providers must be prepared to address it at every delivery.






























































![7-Shoulder_dystocia[1].pptx5555555555555555555555](https://cdn.slidesharecdn.com/ss_thumbnails/7-shoulderdystocia1-240901140722-b7a2771f-thumbnail.jpg?width=640&height=640&fit=bounds)