Downloaded 34 times

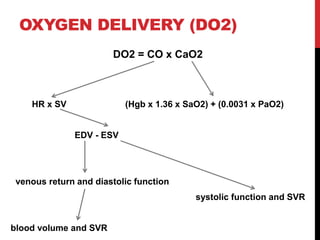
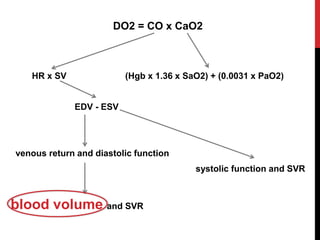

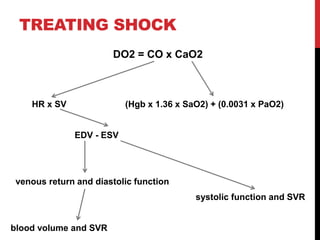



Shock is a life-threatening condition caused by inadequate tissue perfusion and oxygen delivery. Early recognition and treatment is important to prevent progression. The main goals in treating shock are to restore oxygen delivery through fluid resuscitation and addressing the underlying cause. Fluid therapy aims to optimize cardiac output and tissue perfusion, but treating the cause of shock such as hemorrhage, sepsis, or heart failure is also critical for patient survival.






















































































