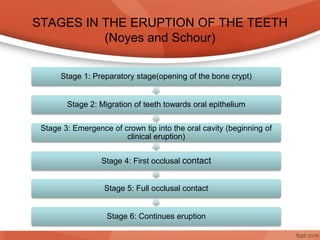
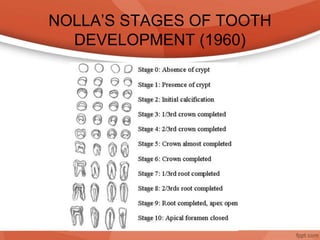
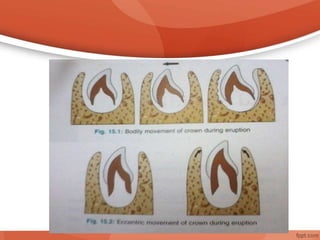
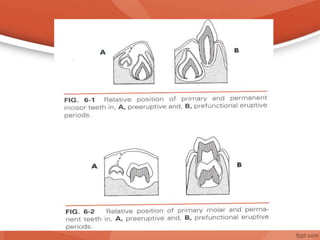
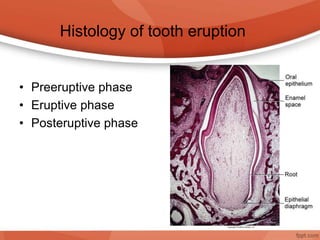
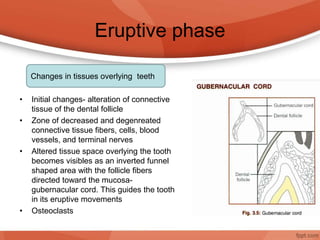
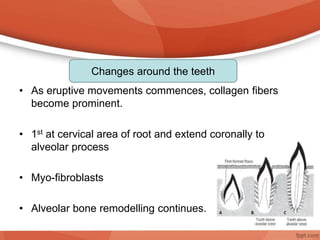
The document details the process of tooth eruption, defining it as the movement of a tooth from its developmental position to its functional position in the oral cavity. It outlines various stages of tooth eruption, including preparatory, eruptive, and post-eruptive phases, as well as the histological changes and theories explaining this process. Additionally, it addresses factors affecting tooth eruption, teething difficulties, natal and neonatal teeth, and systemic conditions that can impact dental development.