Downloaded 71 times
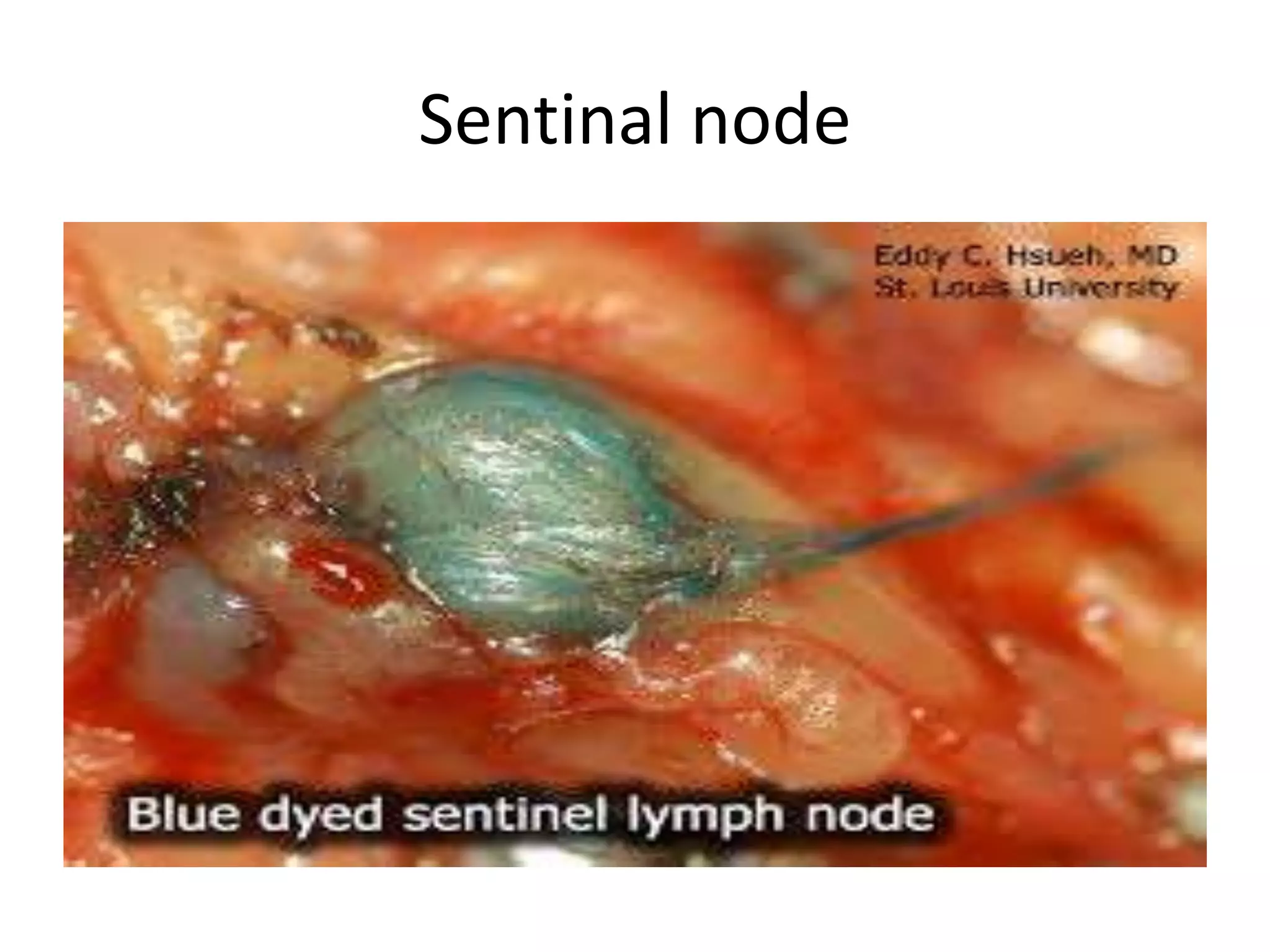
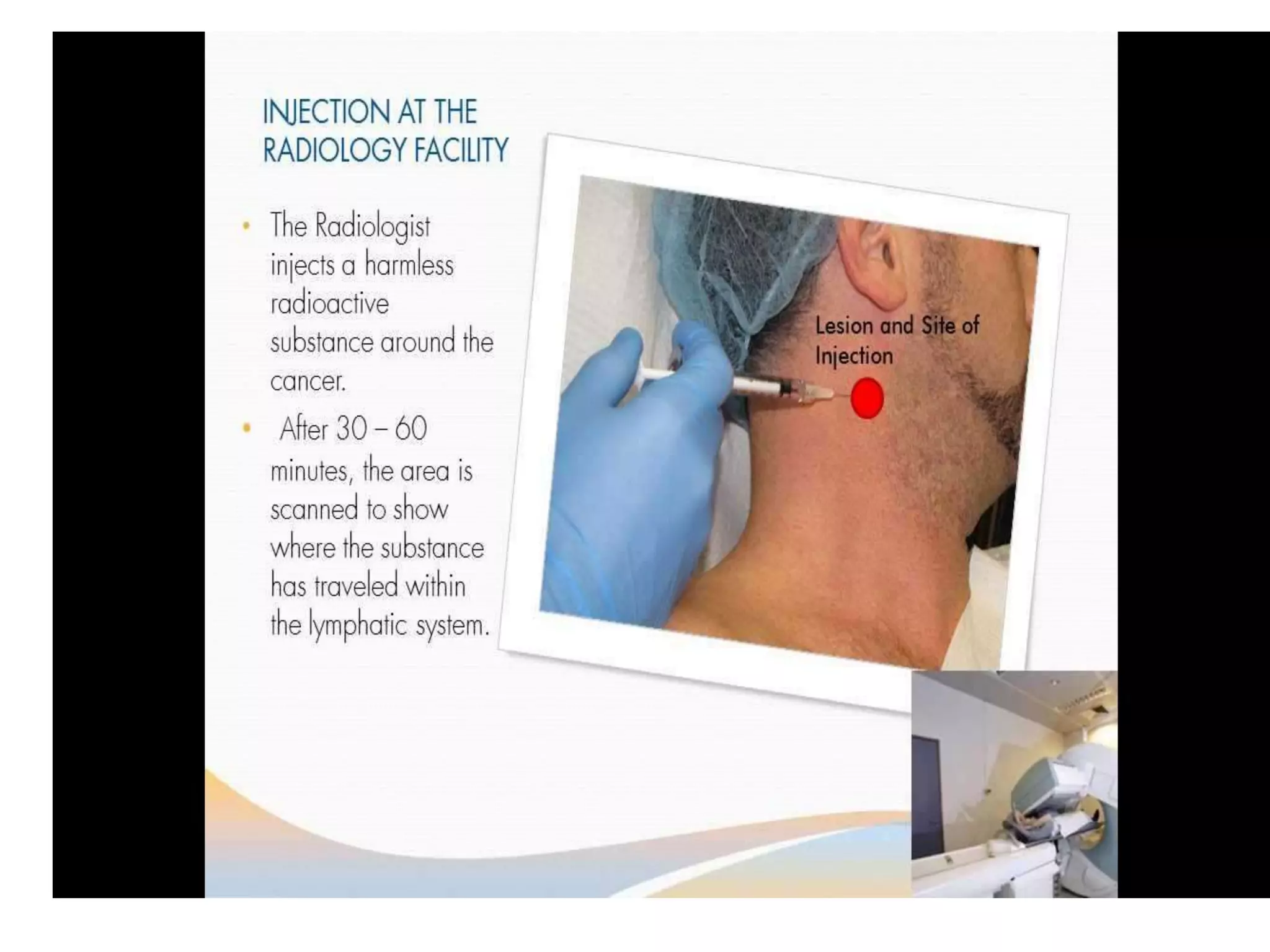
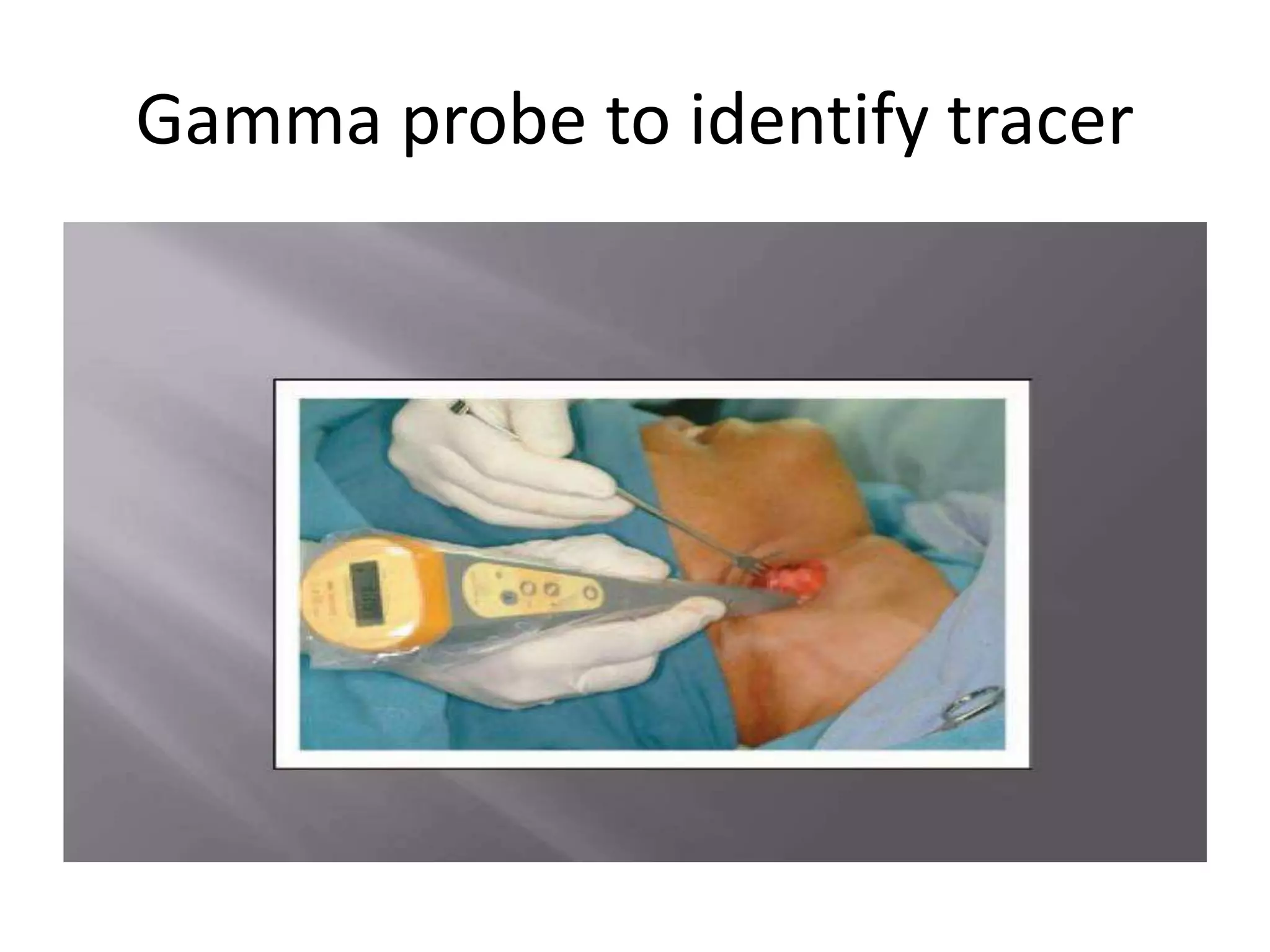
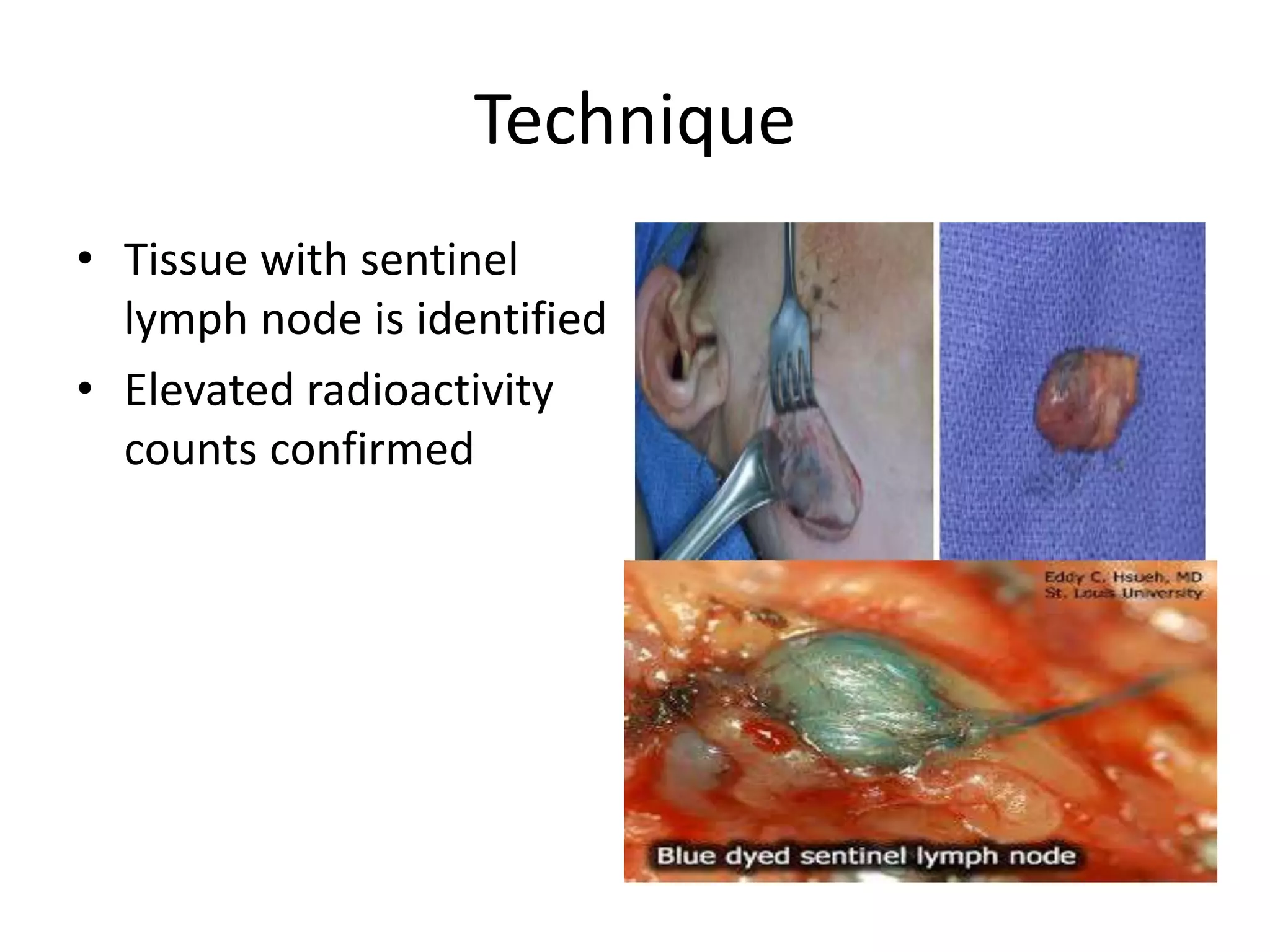
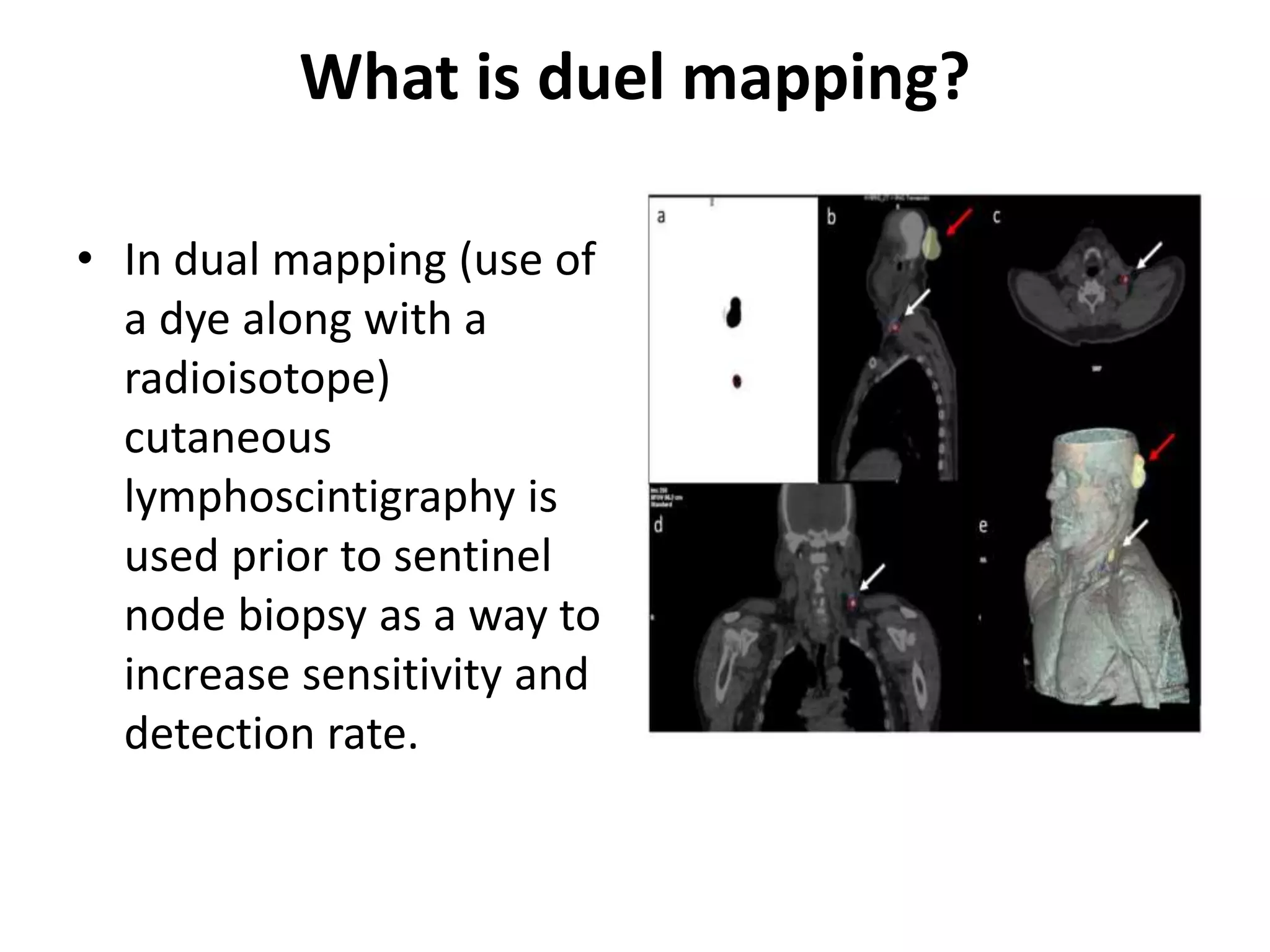


Sentinal lymph node biopsy is a staging procedure used to detect occult metastases in early stage cancers. The sentinel lymph node is the first lymph node to receive drainage from a tumor. During the procedure, a radioactive tracer is injected around the tumor and followed using a gamma probe to identify the sentinel lymph node, which is then surgically removed and examined for cancer cells. Identifying metastases in the sentinel lymph node can help determine the need for further treatment such as neck dissection while avoiding unnecessary procedures in node-negative patients. While controversial in oral cancers due to variability in lymphatic drainage, sentinel lymph node biopsy may help improve staging and individualize treatment when performed by an experienced team.























































































