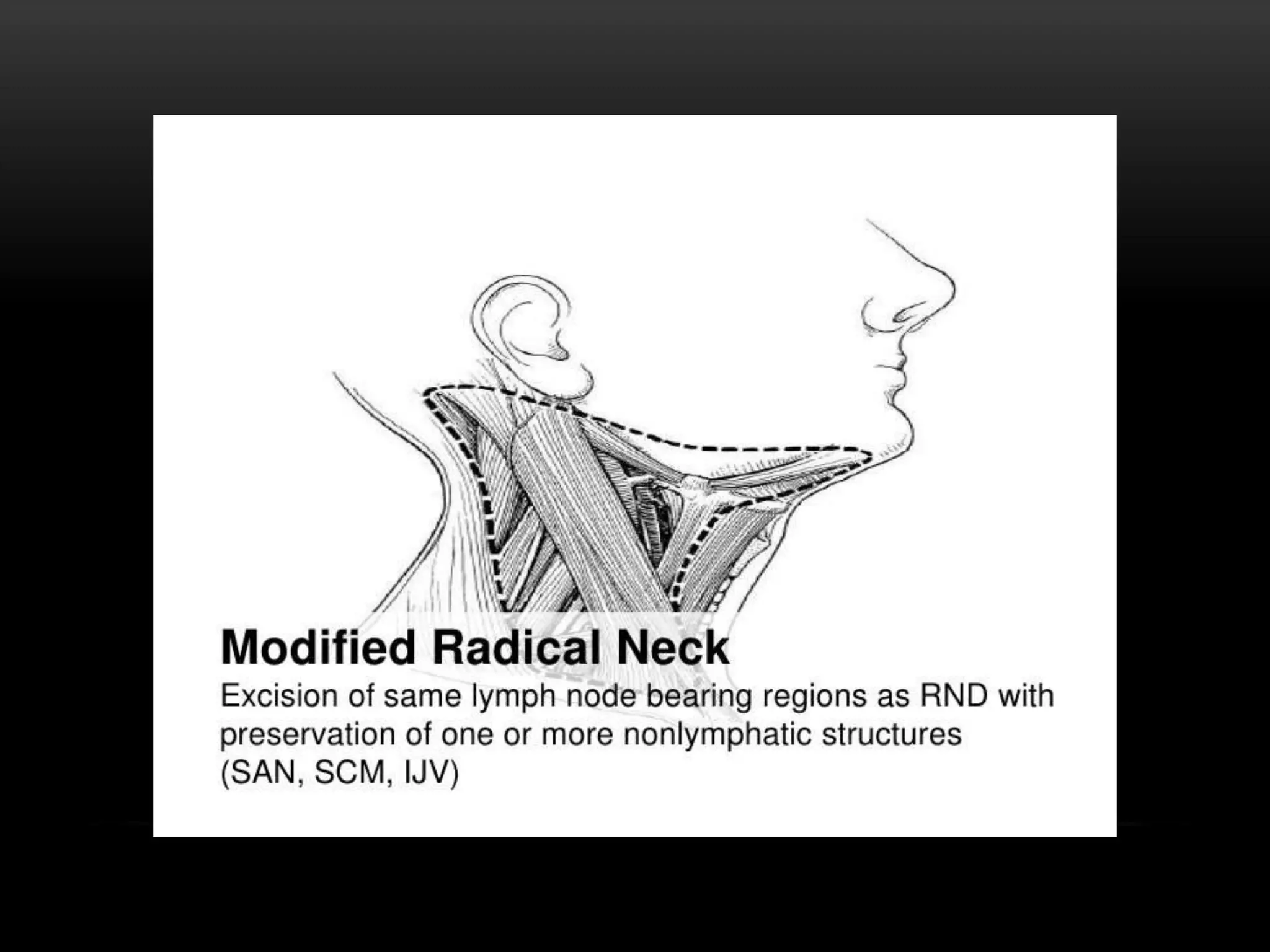
This document discusses types of neck dissection procedures performed to treat neck metastases from head and neck cancers. It describes radical neck dissection, modified radical neck dissection, and selective neck dissection. Radical neck dissection removes all lymph nodes from levels I-V, while modified versions preserve one or more non-lymphatic structures like the spinal accessory nerve or internal jugular vein. Selective neck dissection removes only the lymph nodes at levels that drain the primary tumor site. The indications, techniques, and complications of these neck dissection procedures are examined in detail.