Downloaded 38 times





















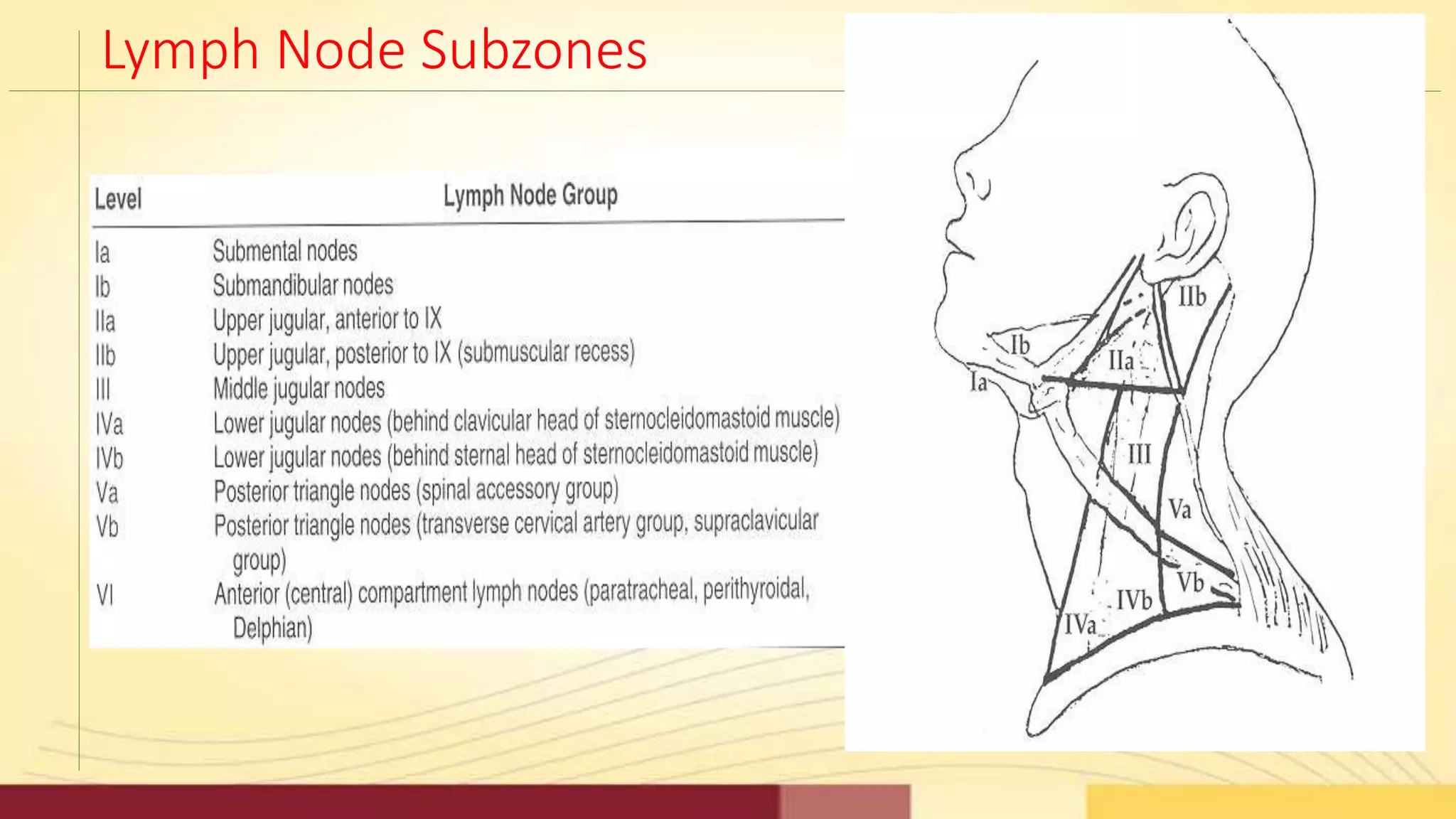






















































































1) Neck dissection refers to surgical removal of lymph nodes and tissue in the neck to treat cervical lymph node metastasis from cancers like head and neck cancers. 2) The procedure has evolved from radical neck dissections removing most neck structures to more selective and modified radical neck dissections that preserve key structures like the spinal accessory nerve and internal jugular vein. 3) Proper classification of neck dissection types and the specific lymph node levels involved is important for standardized reporting and determining prognosis.











































































