Downloaded 1,025 times
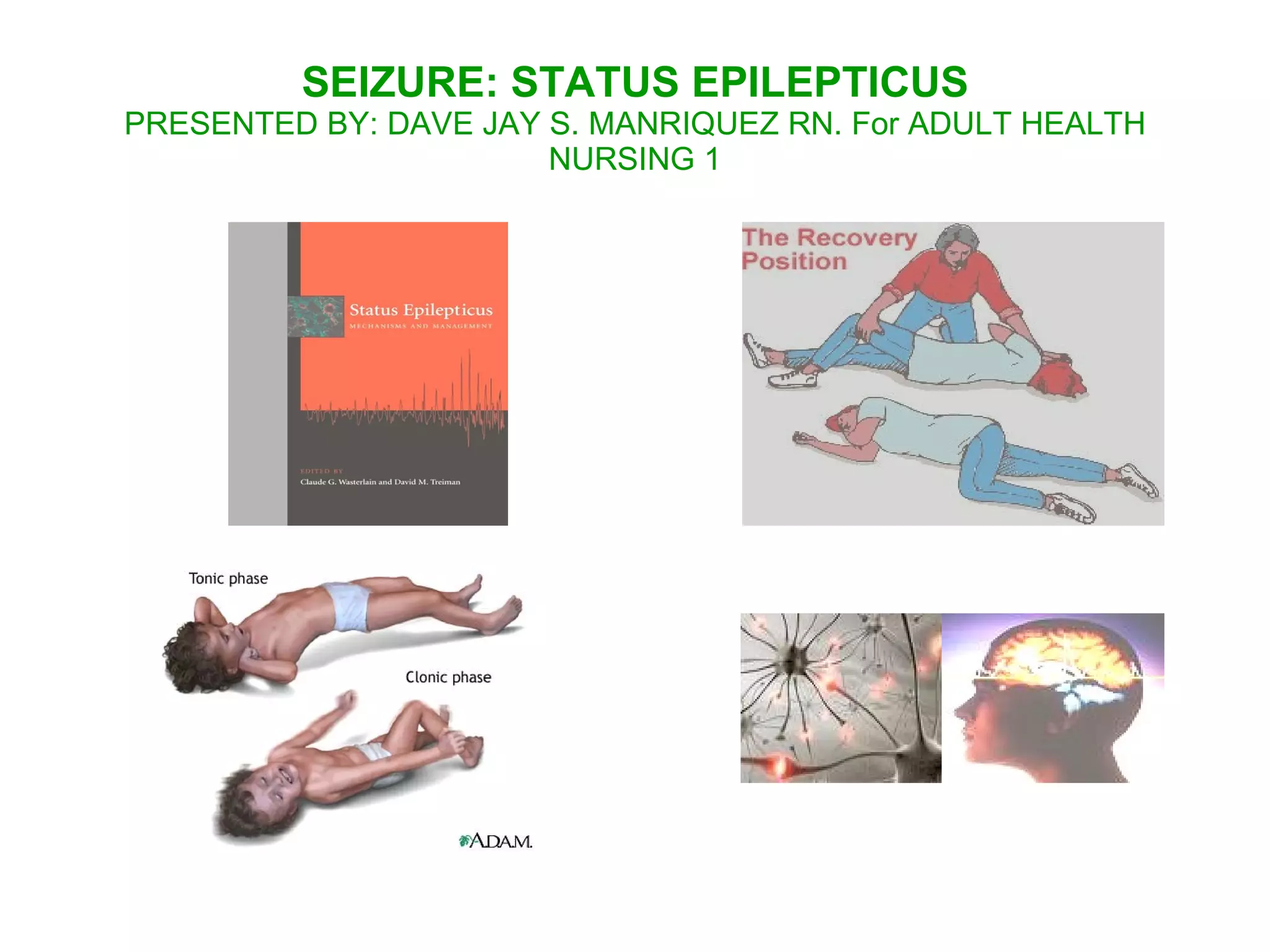

1. Status epilepticus is a medical emergency characterized by prolonged seizures without recovery between seizures or continuous seizure activity lasting more than 30 minutes. 2. It can be caused by not taking anti-seizure medications, infections, brain tumors, head trauma, or other underlying medical conditions. 3. Nursing care focuses on preventing injury during seizures, reducing fears and improving coping, providing education to patients and families, and monitoring for complications of prolonged seizure activity and medication side effects.











































































































