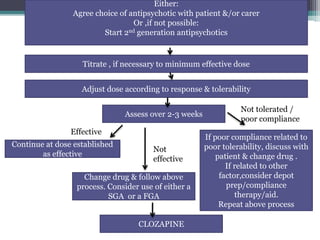
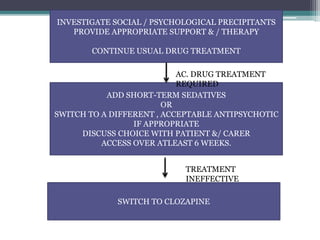
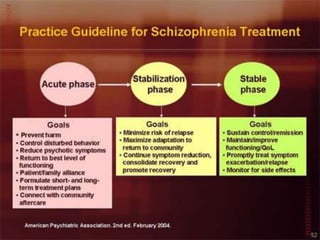
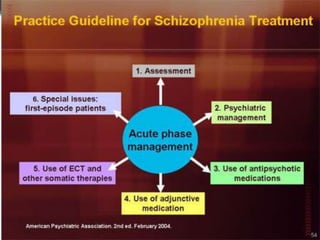
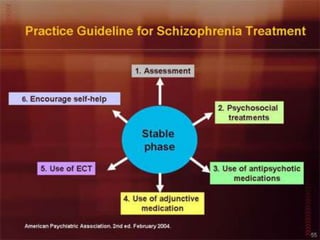
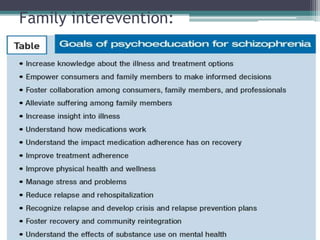
This document summarizes guidelines for managing schizophrenia through pharmacological and psychosocial treatment. It discusses using antipsychotic medications such as second generation antipsychotics for acute episodes and maintaining treatment. Clozapine is recommended for treatment-resistant cases. Psychosocial interventions like family therapy, cognitive behavioral therapy, social skills training, supported employment, and substance abuse rehabilitation are described. Long-acting injectable antipsychotics can help with treatment adherence. The overall goal of management is achieving remission of symptoms and optimal functioning through a combination of medical and psychosocial support.
























































![Management of schizophrenia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/managementofschizophreniaautosaved-201026030437-thumbnail.jpg?width=640&height=640&fit=bounds)

































