Downloaded 150 times
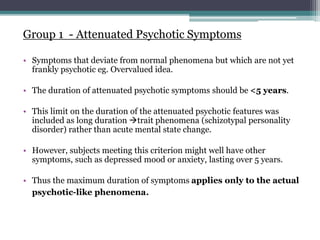
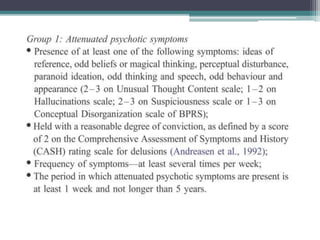
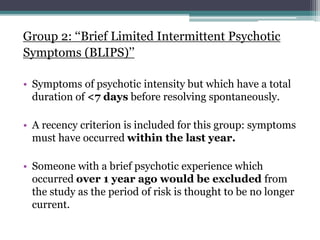
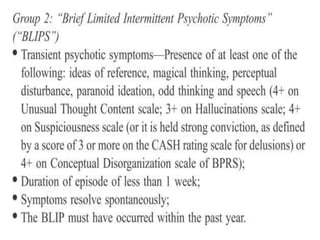
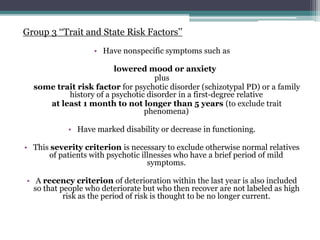
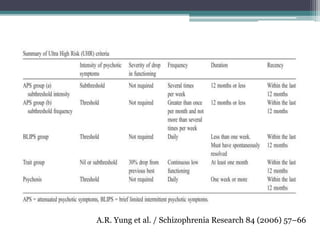
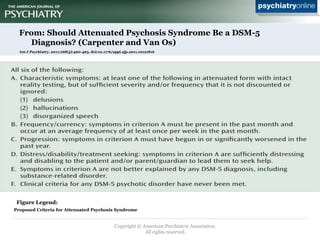

The document discusses the concepts of At Risk Mental State (ARMS), Ultra High Risk (UHR), and Attenuated Psychosis Syndrome. ARMS refers to individuals at risk but not certain to develop psychosis. UHR criteria were introduced to identify those at the highest risk, defined as having attenuated psychotic symptoms, brief intermittent psychotic symptoms, or vulnerability factors plus functional impairment. Studies found 20-40% of UHR individuals developed psychosis within 1-2 years. Basic symptom criteria also predicted increased risk. While Attenuated Psychosis Syndrome was proposed for DSM-5, it was ultimately included only for further study and not as an official diagnosis.





























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













