1. Schizophrenia is a chronic neuropsychiatric disorder affecting about 1% of the world's population that imposes a large economic burden.
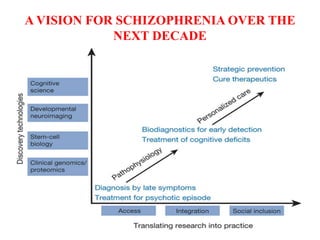
2. While the exact causes remain unclear, current research suggests schizophrenia involves alterations in brain development and circuits during early development. Genetics also play a role as risk factors.
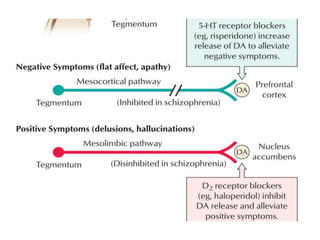
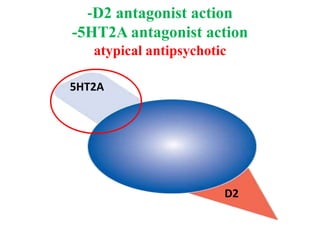
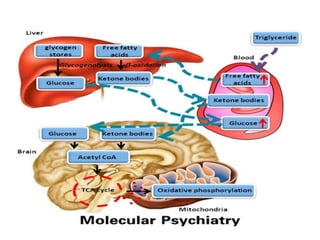
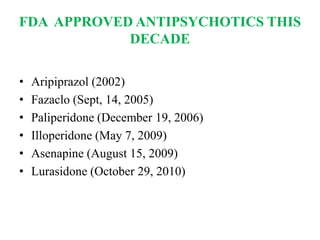
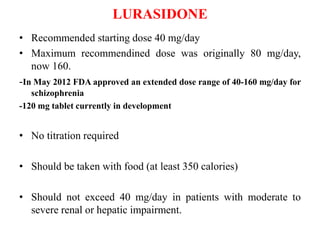
3. Recent advances in treatment include new atypical antipsychotic medications that target both dopamine and serotonin receptors, as well as research into alternative treatments targeting negative symptoms, cognitive impairments, and underlying neuropathology and metabolic abnormalities.




















































![• Lindamer LA, Buse DC, Lohr JB, et al. Hormone replacement therapy in
postmenopausal women with schizophrenia: positive effect on negative
symptoms? Biol Psychiatry. 2001; 49(1):47-51.
• Usall J, Huerta-Ramos, Iniesta R, et al. Raloxifene as Adjunctive Treatment
for Postmenopausal Women with Schizophrenia: A Double-Blind,
Randomized, Placebo-Controlled trial. J Clin Psychiatry 2011;
72(11):15552-1557.
• Kulkarni J, Gurvich C, Lee SJ, et al. Piloting the effective therapeutic dose
of adjunctive selective estrogen receptor modulator treatment in
postmenopausal women with schizophrenia. Psychoneuroendocrinology.
2010;35(8):1142-1147
• Berk M, Munib A, Dean O et al. Qualitative methods in earlyphase drug
trials: data and methods from a trial of N-acetyl cysteine in schizophrenia.
J Clin Psychiatry 2010 Sep. 1 [Epub ahead of print].
• Suzie Lavoie, Micah M Murray , Patricia Deppen, Maria G Knyazeva,
Michael Berk Olivier Boulat, Pierre Bovet, Ashley I Bush, Philippe Conus,
David Copolov, Eleonora Fornari,Reto Meuli, Alessandra Solida, Pascal
Vianin, Michel Cue´nod, Thierry Buclin and Kim Q Glutathione Precursor,
N-Acetyl-Cysteine, Improves Mismatch Negativity in Schizophrenia
Patients. Neuropsychopharmacology (2008) 33, 2187–2199.](https://image.slidesharecdn.com/advancesinschizophrenia-170224102344/85/Advances-in-schizophrenia-92-320.jpg)










































































