Downloaded 242 times


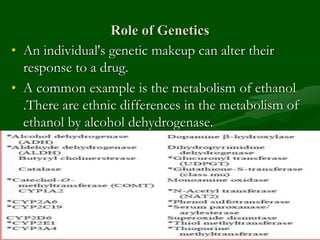
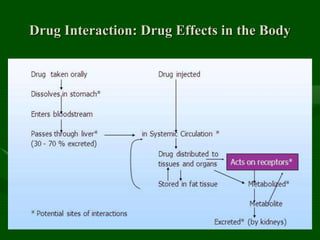
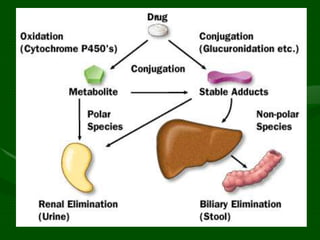
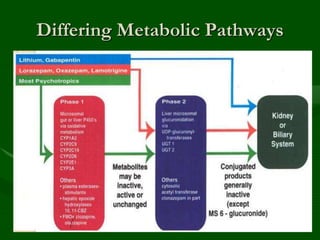
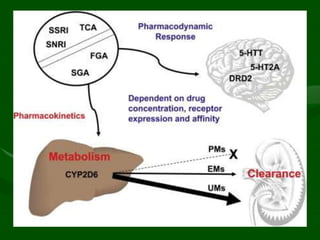
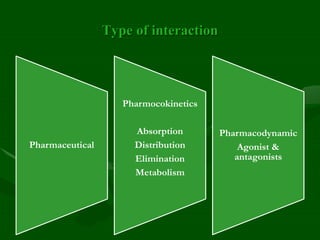
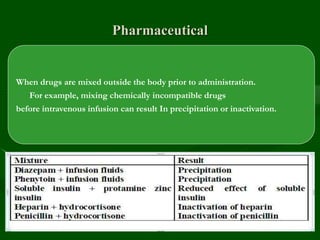
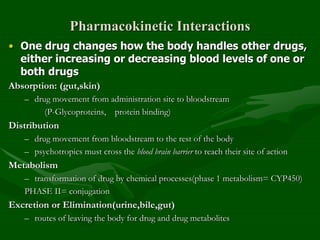
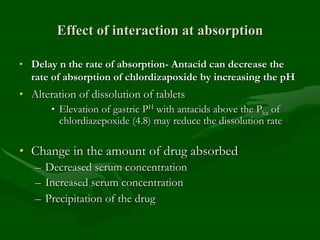
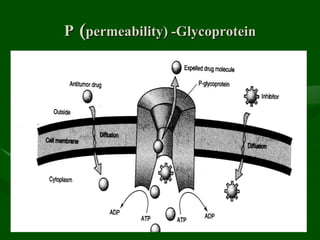
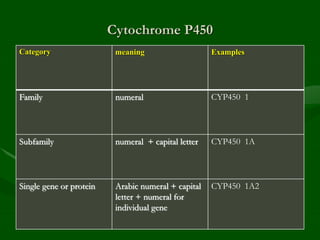
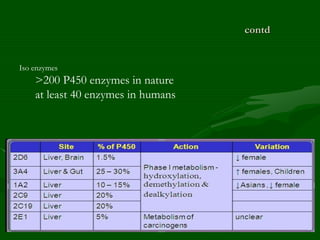
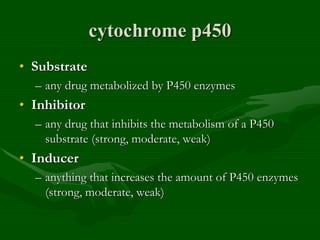
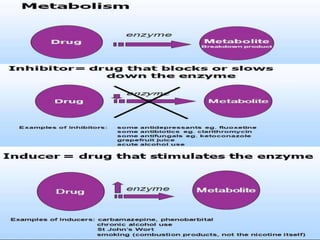
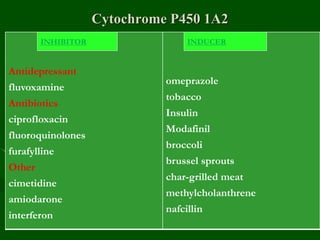
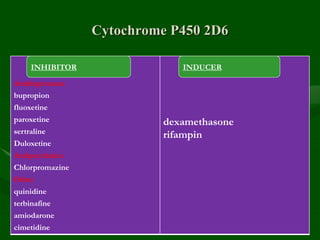

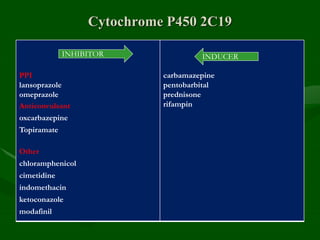
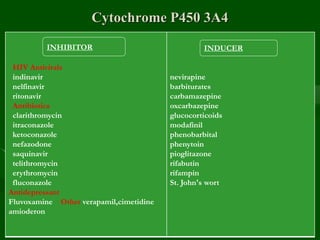
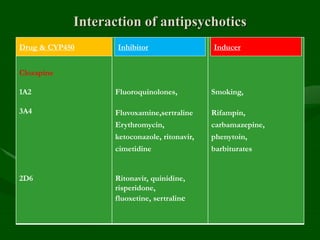
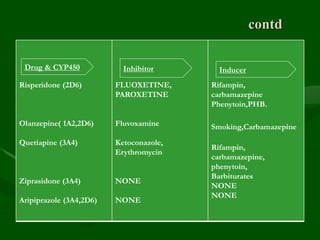
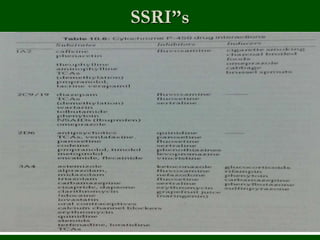
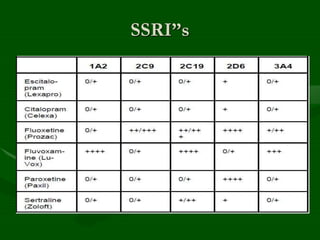

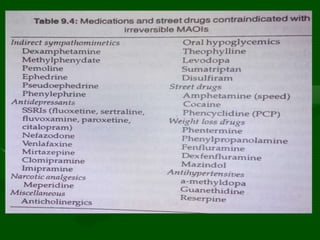


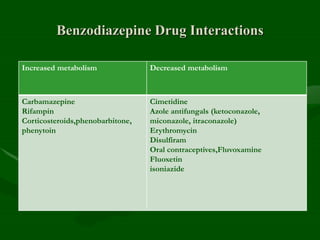


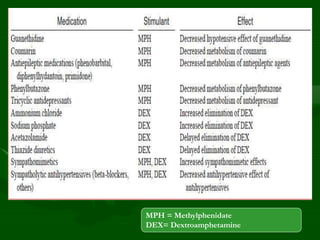
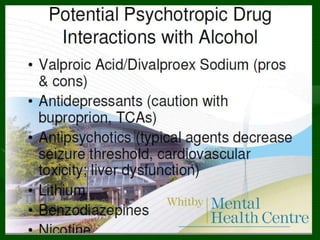
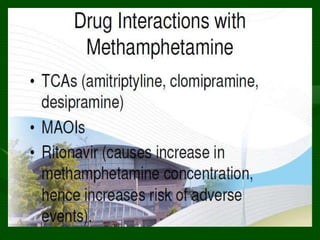

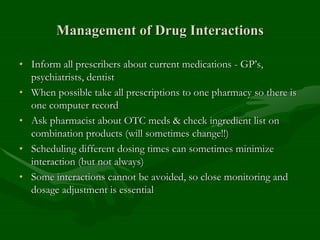


Drug interactions are an important consideration in psychiatry. Several types of interactions can occur, including pharmaceutical, pharmacokinetic, and pharmacodynamic. Pharmacokinetic interactions can affect absorption, distribution, metabolism, and excretion of drugs. Many psychiatric medications are substrates, inhibitors, or inducers of cytochrome P450 enzymes, particularly CYP1A2, CYP2D6, CYP2C9, CYP2C19, and CYP3A4. Recognition of interactions is important to avoid adverse effects or lack of efficacy. Management may require dosage adjustments or choosing alternative medications.



![Principles of psychopharm[1]](https://cdn.slidesharecdn.com/ss_thumbnails/principlesofpsychopharm1-111129095442-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



















































































