This document summarizes information about malaria in Bangladesh, including:
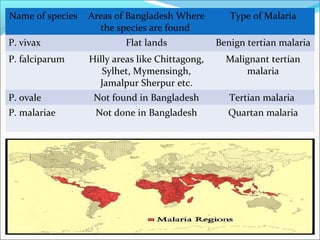
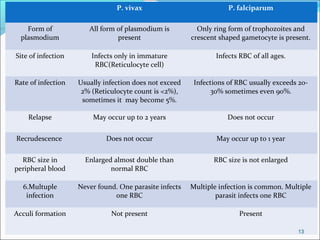
- The main Plasmodium species that cause malaria in different regions of Bangladesh. P. vivax causes benign tertian malaria in flat lands, while P. falciparum causes malignant tertian malaria in hilly areas.
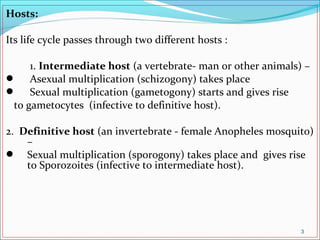
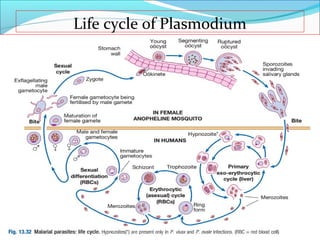
- The life cycle of Plasmodium, which involves both an intermediate human host and definitive mosquito host.
- The pathogenesis of malaria, including the infective forms, hosts, vectors, reservoirs, and modes of transmission.
- The clinical features of malaria, including periodic fevers, anemia, splenomegaly, and potential complications like cerebral malaria and blackwater fever.
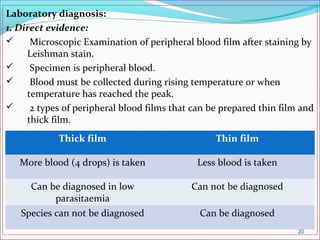
- Methods for laboratory