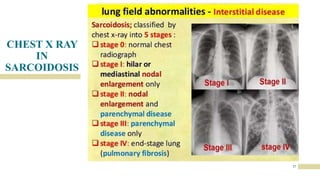
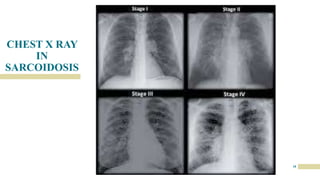
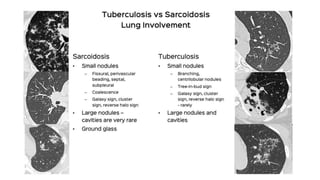
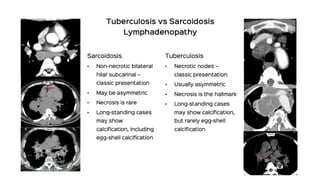
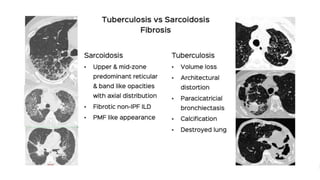
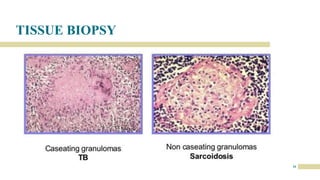
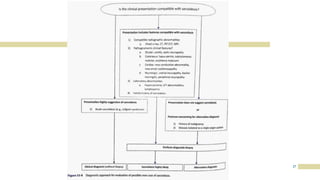
This document provides an overview of the similarities and differences between sarcoidosis and pulmonary tuberculosis, two granulomatous lung diseases that can be difficult to distinguish. Both commonly present with nonspecific constitutional symptoms but sarcoidosis typically causes a dry cough and fatigue, while tuberculosis often presents with a cough producing sputum and evening fevers. Diagnosis of sarcoidosis relies on biopsy evidence of non-caseating granulomas and usually excludes tuberculosis, whereas tuberculosis diagnosis requires identification of Mycobacterium tuberculosis via smear, culture or molecular testing. Distinguishing the two is important for determining appropriate treatment with corticosteroids or anti-tubercular drugs, respectively.