Download as PDF, PPTX




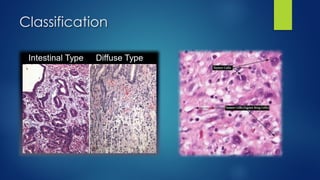






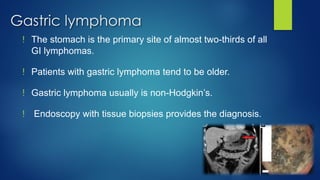


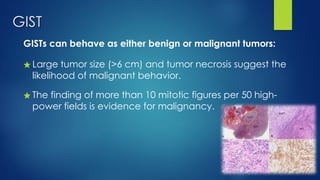


Malignant gastric tumors include gastric cancer and gastric lymphoma. Gastric cancer is the sixth most common cancer worldwide and risk factors include H. pylori infection and pernicious anemia. Early cancers are often asymptomatic, while advanced cancers present with vague epigastric pain, weight loss, dysphagia, bleeding, or anemia. Diagnosis involves endoscopy with biopsy for histology. Treatment is surgical resection with chemotherapy and radiation for localized disease. Gastric lymphoma presents similarly and is diagnosed with endoscopy and biopsy. Treatment involves chemotherapy alone. Gastrointestinal stromal tumors (GISTs) are submucosal gastric masses that may behave benignly or malignantly depending on size and mitotic rate



























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







