Download to read offline



















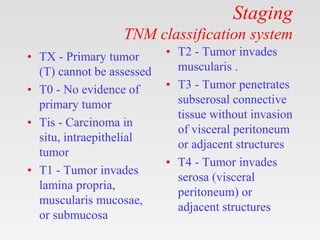
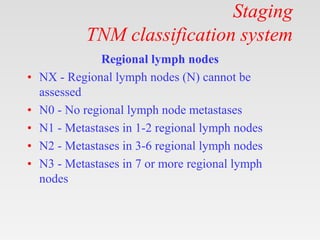




















This document provides tips and guidelines for using a PowerPoint presentation on stomach cancer. It includes 12 slides on topics like introduction/history, etiology, anatomy, pathology, staging, classification, investigations, management, prevention, and guidelines. The document recommends using blank slides to engage students in an active learning session by asking them questions before presenting content. It also notes the presentation is good for self-study and refers the user to notes for bibliography citations.



































































