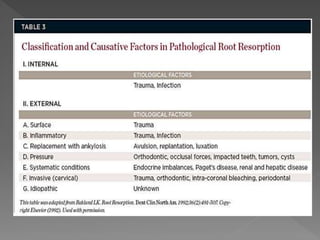
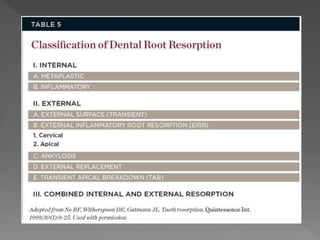
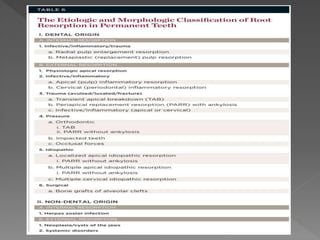
This document discusses root resorption, which is the loss of tooth structure due to clastic cells called odontoclasts. It can be physiologic during primary tooth exfoliation or pathologic in permanent teeth. Pathologic resorption includes internal resorption within the root canal from pulp inflammation and external resorption on root surfaces. The mechanism involves odontoclasts resorbing both inorganic and organic tooth structure. Treatment depends on the type and extent but often involves root canal therapy, repair of resorptive defects, and monitoring for signs of reoccurrence.