Resorption – Dr.Nithin Mathew
Internal Resorption
• Definition:
• Internal resorption is an unusual form of tooth resorption that begins centrally
within the tooth, apparently initiated in most cases by a peculiar inflammation of
the pulp
• Internal Root Resorption
• Internal surface resorption
• Internal infection related root resorption
• Internal replacement resorption
[ Shafer ]
[ Ingle ]
3.
Resorption – Dr.Nithin Mathew
Internal Resorption
Clinical Features:
• Asymptomatic until it has perforated and become necrotic
• Detected through routine radiographs
• Pain : lesion perforates and tissue exposed to oral fluids
• Can be found in all areas of root but most commonly found in cervical region
• Common in maxillary central incisors
• Usually single tooth but can involve multiple teeth
• Granulation tissue manifests as a “Pink Spot”
[ Ingle ]
Resorption – Dr.Nithin Mathew
Internal Surface Resorption
Etiology:
• Found in areas where revascularisation occurs
• Fracture lines of root fracture
• Apical part of root canal of luxated teeth undergoing revascularisation
Pathogenesis:
• Osteoclastic activity is part of the process along with formation of granulation
tissue
[ Ingle ]
6.
Resorption – Dr.Nithin Mathew
Internal Surface Resorption
Radiographic Findings:
• Appears to be a temporary widening of root canal
Endodontic Implications:
• Resorption process - is a sign of progressing pulp healing.
• Any endodontic intervention may arrest this process.
Treatment:
• No treatment except periodic observation
[ Ingle ]
7.
Resorption – Dr.Nithin Mathew
Transient Apical Internal Resorption
• Another form of trauma induced non-infective root resorption identified by Andreasen in 1986.
• Resorption follow luxation injuries
• Recognized by a confined periapical radiolucency which resolves within a few months.
• There may be associated colour change due to intra-pulpal haemorrhage.
• This resolve spontaneously if revascularisation to the coronal pulp chamber occurs
[ Australian Dental Journal Endodontic 2007 ]
8.
Resorption – Dr.Nithin Mathew
Transient Apical Internal Resorption
• In the longer term, (transient process), the internally resorbed apex will close uneventfully.
[ Australian Dental Journal Endodontic 2007 ]
Radiograph taken 1 year after the original
trauma shows resolution of the apical
internal resorption and no other signs of
periradicular pathosis
Resorption – Dr.Nithin Mathew
Internal Infection Related Root Resorption
Etiology:
• Coronal to the resorption site in pulp, necrotic infected tissue is
found.
• Resorption site – represents resorbing granulation tissue
interposed between healthy & diseased pulp
Pathogenesis:
• Resorption process – gradually expand – leading to fracture of
root
119
[ Ingle ]
11.
Resorption – Dr.Nithin Mathew
Internal Infection Related Root Resorption
Treatment:
• Endodontic treatment is appropriate
• Require technique that allows management of resorbed area
• Thermoplastic obturation
[ Ingle ]
12.
Resorption – Dr.Nithin Mathew
Internal Infection Related Root Resorption
• Internal inflammatory resorption may be classified according to location :
• Apical
• Intraradicular
Apical :
• Study showed that 74.7 % of teeth with periapical lesions had varying
degrees of apical internal resorption.
• Radiographically, apical internal resorption is difficult to diagnose when
the resorptions are of the lower grades.
[ Int Endod J 2004;37 ]
[ Australian Dental Journal Endodontic 2007 ]
13.
Resorption – Dr.Nithin Mathew
Internal Infection Related Root Resorption
Intraradicular :
• Internal resorption fully contained within an intact root
• Round or oval shaped radiolucencies contained within the tooth root
14.
Resorption – Dr.Nithin Mathew
Internal Infection Related Root Resorption
Treatment:
• Defect not perforated the root to the periodontal ligament :
• Obturation with warm guttapercha technique.
• Defect perforated the root below bone level :
• A hard tissue barrier can be produced with long-term calcium hydroxide treatment,
after which obturation is carried out.
• Defect perforates coronal to the epithelial attachment or if an extremely large perforation is
present :
• A surgical approach is required to seal the perforation.
[ Cohen ]
15.
Resorption – Dr.Nithin Mathew
Internal Infection Related Root Resorption
Treatment (Apical) :
• Extend instrumentation only to the position of the resorption.
• With the removal of micro-organisms followed by root canal filling,
hard tissue repair will occur in the resorbed apical region.
• Treatment to the position of the resorption help in achieving biological
repair of the resorbed apex.
[ Australian Dental Journal Endodontic 2007 ]
Radiograph taken 2 years later showing
periradicular repair and control of the root
resorption.
16.
Resorption – Dr.Nithin Mathew
Internal Infection Related Root Resorption
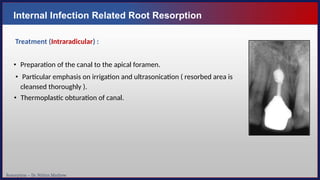
Treatment (Intraradicular) :
• Preparation of the canal to the apical foramen.
• Particular emphasis on irrigation and ultrasonication ( resorbed area is
cleansed thoroughly ).
• Thermoplastic obturation of canal.
Resorption – Dr.Nithin Mathew
Internal Replacement Resorption
Etiology:
• Damage to pulp tissue usually related to trauma.
• When damaged pulp tissue replaced as a part of healing process – tissue
metaplasia occurs – formation of bone tissue in pulp canal
• Damaged pulp tissue – replaced with an ingrowth of new tissue, includes
bone derived cells.
Pathogenesis:
• Root will gradually be replaced with bone
• In some cases bone replacement will spontaneously arrest
[ Ingle ]
Resorption – Dr.Nithin Mathew
Internal Replacement Resorption
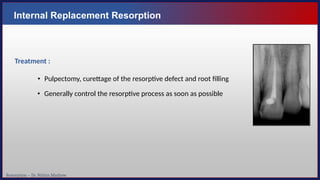
Treatment :
• Pulpectomy, curettage of the resorptive defect and root filling
• Generally control the resorptive process as soon as possible
21.
Resorption – Dr.Nithin Mathew
Internal Replacement Resorption
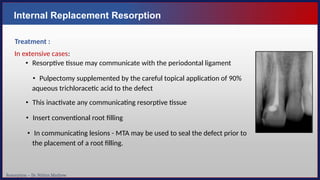
Treatment :
In extensive cases:
• Resorptive tissue may communicate with the periodontal ligament
• Pulpectomy supplemented by the careful topical application of 90%
aqueous trichloracetic acid to the defect
• This inactivate any communicating resorptive tissue
• Insert conventional root filling
• In communicating lesions - MTA may be used to seal the defect prior to
the placement of a root filling.
22.
Resorption – Dr.Nithin Mathew
Physiologic Root Resorption
• Entirely normal process
• Happens with the timely loss of deciduous teeth
• Occurs during the exfoliation of the primary dentition and eruption of
permanent successors
• Occurs in three separate phases
• Active
• Partial
• Reparative
23.
Resorption – Dr.Nithin Mathew
Pathologic Resorption due to Systemic Causes
• Resorption occurs at the apex of several teeth and is bilateral
• Hypo parathyroidism
• Hyper parathyroidism
• Calcinosis
• Turner’s syndrome
• Paget’s disease
• Following radiotherapy
• Renal distrophy
• Genetic factors
24.
Resorption – Dr.Nithin Mathew
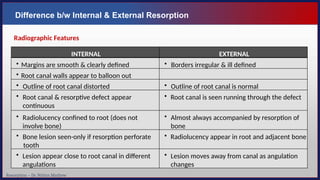
Difference b/w Internal & External Resorption
INTERNAL EXTERNAL
• Margins are smooth & clearly defined • Borders irregular & ill defined
• Root canal walls appear to balloon out
• Outline of root canal distorted • Outline of root canal is normal
• Root canal & resorptive defect appear
continuous
• Root canal is seen running through the defect
• Radiolucency confined to root (does not
involve bone)
• Almost always accompanied by resorption of
bone
• Bone lesion seen-only if resorption perforate
tooth
• Radiolucency appear in root and adjacent bone
• Lesion appear close to root canal in different
angulations
• Lesion moves away from canal as angulation
changes
Radiographic Features
25.
Resorption – Dr.Nithin Mathew
Pharmacological Management of Inflammatory Response
• Drugs that affects osteoclasts present at the site of resorption :
• Tetracyclines
• Sustained antimicrobial effect
• Anti-resorptive properties
• Direct inhibitory effect on osteoclasts and collagenase
• Significantly more cemental healing
• Drugs that affect the recruitment of osteoclasts to the injury site :
• Glucocorticoids
• Topical dexamethasone was found to be useful while systemic usage was not
• Bisphoshonates
• Alendronate
• Amino acids
• Taurine
26.
Resorption – Dr.Nithin Mathew
Pharmacological Management of Inflammatory Response
• Combination of the two types of drugs
• Synergistic effect on the inhibition of root resorption
• Ledermix
• A drug combining tetracycline and corticosteroids
27.
Resorption – Dr.Nithin Mathew
ART - Antiresorptive Regenerative Therapy (Pohl et al 2005)
• Comprises a combination of different treatment strategies for a synergistic effect :
• Local application of a glucocorticoid
• Systemic and local application of Tetracyclines
• Use of Enamel Matrix Derivative (EMD) e.g. Emdogain
• Emdogain (Enamel Matrix Protein)
•Makes the root more resistant to resorption
•Stimulates the formation of new periodontal ligament from the socket
28.
Resorption – Dr.Nithin Mathew
AAE Guidelines (Management of External Root Resorption)
Unfavorable:
Structural integrity of the tooth or
root is compromised
• There are deep probing depths
associated with the resorptive
defect
• The defect is not accessible for
repair surgically
Favorable:
Minimal loss of tooth structure
• Located cervically but above
the crestal bone
• The lesion
repair
is accessible for
• Apical
associated
root
with
resorption
a tooth
exhibiting pulp necrosis and
apical pathosis
Questionable:
Minimal impact on restorability of
tooth
• Crown lengthening or
orthodontic root extrusion may
be required
• The pulp may be vital or necrotic
29.
Resorption – Dr.Nithin Mathew
Conclusion
• The diagnosis of dental resorptions and an understanding of the underlying pathosis is critical to
clinical management.
• Most infection related resorption respond well to endodontic treatment.
• Early diagnosis and prompt treatment are the key factors which determine the success of the
treatment.


![Resorption – Dr. Nithin Mathew
Internal Resorption
• Definition:
• Internal resorption is an unusual form of tooth resorption that begins centrally
within the tooth, apparently initiated in most cases by a peculiar inflammation of
the pulp
• Internal Root Resorption
• Internal surface resorption
• Internal infection related root resorption
• Internal replacement resorption
[ Shafer ]
[ Ingle ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-2-320.jpg)
![Resorption – Dr. Nithin Mathew
Internal Resorption
Clinical Features:
• Asymptomatic until it has perforated and become necrotic
• Detected through routine radiographs
• Pain : lesion perforates and tissue exposed to oral fluids
• Can be found in all areas of root but most commonly found in cervical region
• Common in maxillary central incisors
• Usually single tooth but can involve multiple teeth
• Granulation tissue manifests as a “Pink Spot”
[ Ingle ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-3-320.jpg)

![Resorption – Dr. Nithin Mathew
Internal Surface Resorption
Etiology:
• Found in areas where revascularisation occurs
• Fracture lines of root fracture
• Apical part of root canal of luxated teeth undergoing revascularisation
Pathogenesis:
• Osteoclastic activity is part of the process along with formation of granulation
tissue
[ Ingle ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-5-320.jpg)
![Resorption – Dr. Nithin Mathew
Internal Surface Resorption
Radiographic Findings:
• Appears to be a temporary widening of root canal
Endodontic Implications:
• Resorption process - is a sign of progressing pulp healing.
• Any endodontic intervention may arrest this process.
Treatment:
• No treatment except periodic observation
[ Ingle ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-6-320.jpg)
![Resorption – Dr. Nithin Mathew
Transient Apical Internal Resorption
• Another form of trauma induced non-infective root resorption identified by Andreasen in 1986.
• Resorption follow luxation injuries
• Recognized by a confined periapical radiolucency which resolves within a few months.
• There may be associated colour change due to intra-pulpal haemorrhage.
• This resolve spontaneously if revascularisation to the coronal pulp chamber occurs
[ Australian Dental Journal Endodontic 2007 ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-7-320.jpg)
![Resorption – Dr. Nithin Mathew
Transient Apical Internal Resorption
• In the longer term, (transient process), the internally resorbed apex will close uneventfully.
[ Australian Dental Journal Endodontic 2007 ]
Radiograph taken 1 year after the original
trauma shows resolution of the apical
internal resorption and no other signs of
periradicular pathosis](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-8-320.jpg)

![Resorption – Dr. Nithin Mathew
Internal Infection Related Root Resorption
Etiology:
• Coronal to the resorption site in pulp, necrotic infected tissue is
found.
• Resorption site – represents resorbing granulation tissue
interposed between healthy & diseased pulp
Pathogenesis:
• Resorption process – gradually expand – leading to fracture of
root
119
[ Ingle ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-10-320.jpg)
![Resorption – Dr. Nithin Mathew
Internal Infection Related Root Resorption
Treatment:
• Endodontic treatment is appropriate
• Require technique that allows management of resorbed area
• Thermoplastic obturation
[ Ingle ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-11-320.jpg)
![Resorption – Dr. Nithin Mathew
Internal Infection Related Root Resorption
• Internal inflammatory resorption may be classified according to location :
• Apical
• Intraradicular
Apical :
• Study showed that 74.7 % of teeth with periapical lesions had varying
degrees of apical internal resorption.
• Radiographically, apical internal resorption is difficult to diagnose when
the resorptions are of the lower grades.
[ Int Endod J 2004;37 ]
[ Australian Dental Journal Endodontic 2007 ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-12-320.jpg)
![Resorption – Dr. Nithin Mathew
Internal Infection Related Root Resorption
Treatment:
• Defect not perforated the root to the periodontal ligament :
• Obturation with warm guttapercha technique.
• Defect perforated the root below bone level :
• A hard tissue barrier can be produced with long-term calcium hydroxide treatment,
after which obturation is carried out.
• Defect perforates coronal to the epithelial attachment or if an extremely large perforation is
present :
• A surgical approach is required to seal the perforation.
[ Cohen ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-14-320.jpg)
![Resorption – Dr. Nithin Mathew
Internal Infection Related Root Resorption
Treatment (Apical) :
• Extend instrumentation only to the position of the resorption.
• With the removal of micro-organisms followed by root canal filling,
hard tissue repair will occur in the resorbed apical region.
• Treatment to the position of the resorption help in achieving biological
repair of the resorbed apex.
[ Australian Dental Journal Endodontic 2007 ]
Radiograph taken 2 years later showing
periradicular repair and control of the root
resorption.](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-15-320.jpg)
![Resorption – Dr. Nithin Mathew
Internal Replacement Resorption
Etiology:
• Damage to pulp tissue usually related to trauma.
• When damaged pulp tissue replaced as a part of healing process – tissue
metaplasia occurs – formation of bone tissue in pulp canal
• Damaged pulp tissue – replaced with an ingrowth of new tissue, includes
bone derived cells.
Pathogenesis:
• Root will gradually be replaced with bone
• In some cases bone replacement will spontaneously arrest
[ Ingle ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-18-320.jpg)
![Resorption – Dr. Nithin Mathew
Internal Replacement Resorption
Clinical Findings:
• Teeth asymptomatic
• If ankylosis develop – teeth gradually develop infraocclusion
Radiographic Findings:
• A dissecting resorptive area- seen in root canal initially
• Root canal appears intact
[ Ingle ]](https://image.slidesharecdn.com/25601273-250312212841-0b46096a/85/25601273-pptx-resoption-in-endodontic-work-19-320.jpg)