The document provides guidance on safely transferring patients from one surface to another. It describes different types of transfers that vary based on a patient's abilities and needs. Key points include:
1) Assessing a patient's physical, cognitive, and medical status is important for determining the best transfer method.
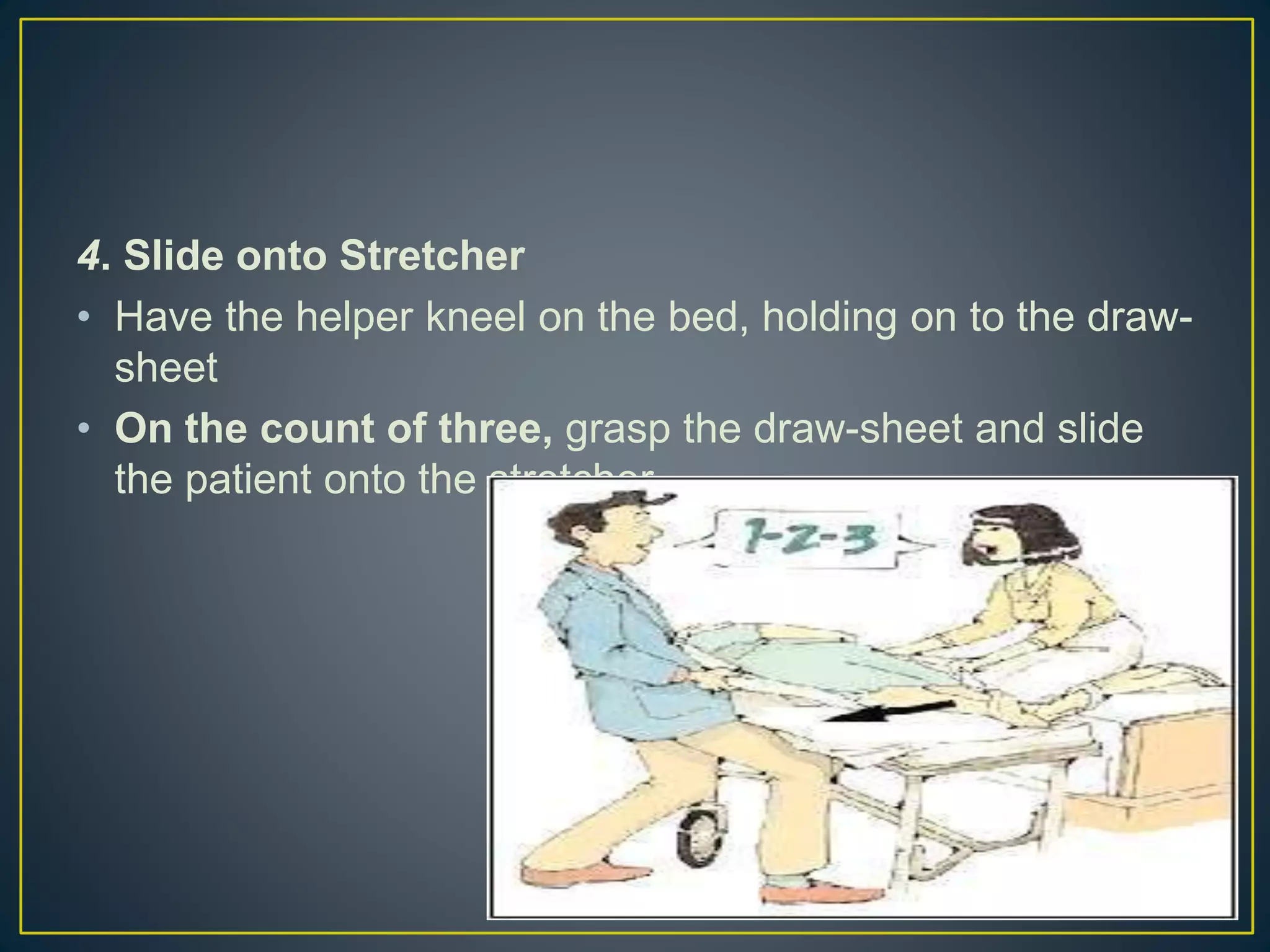
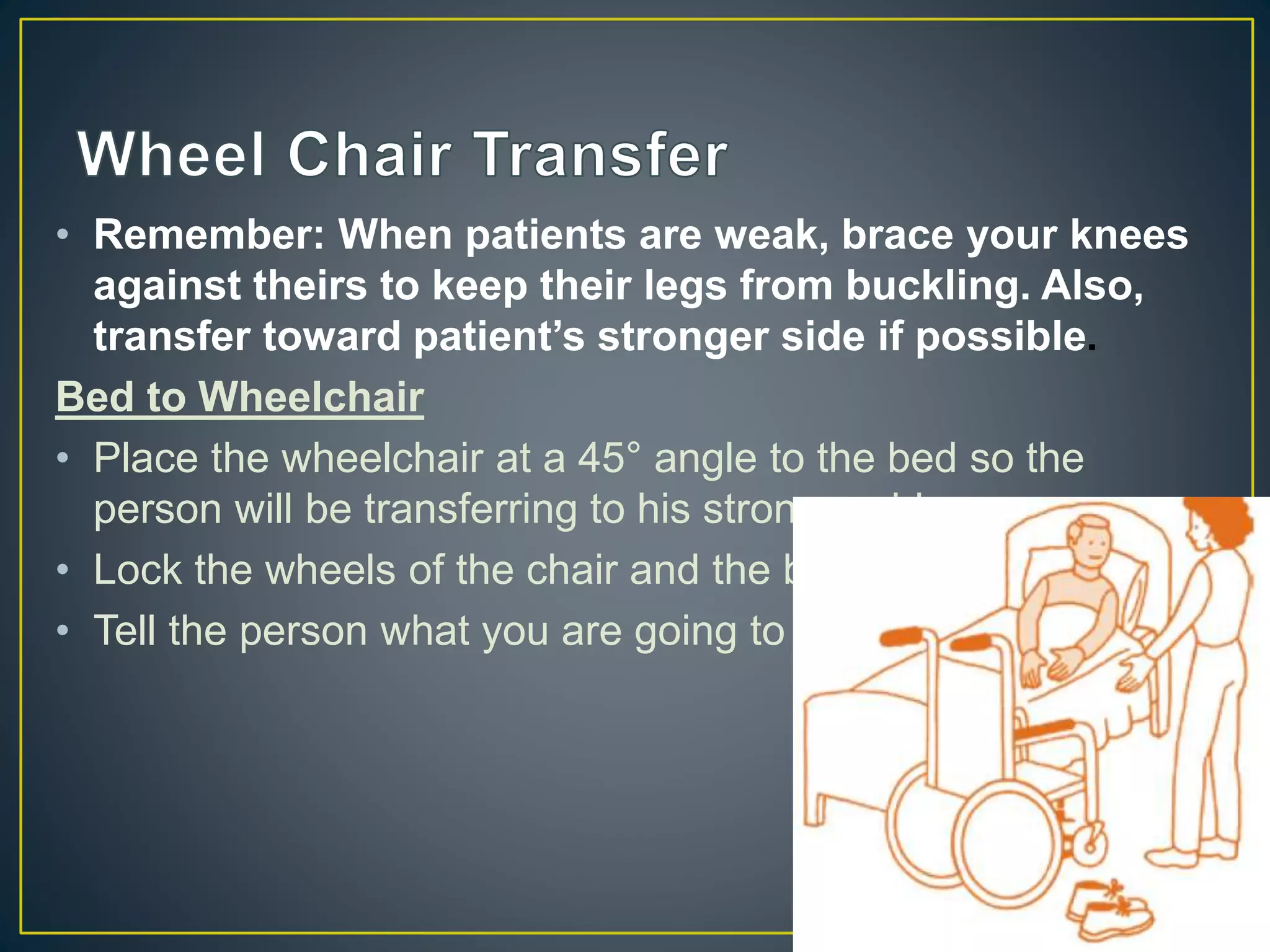
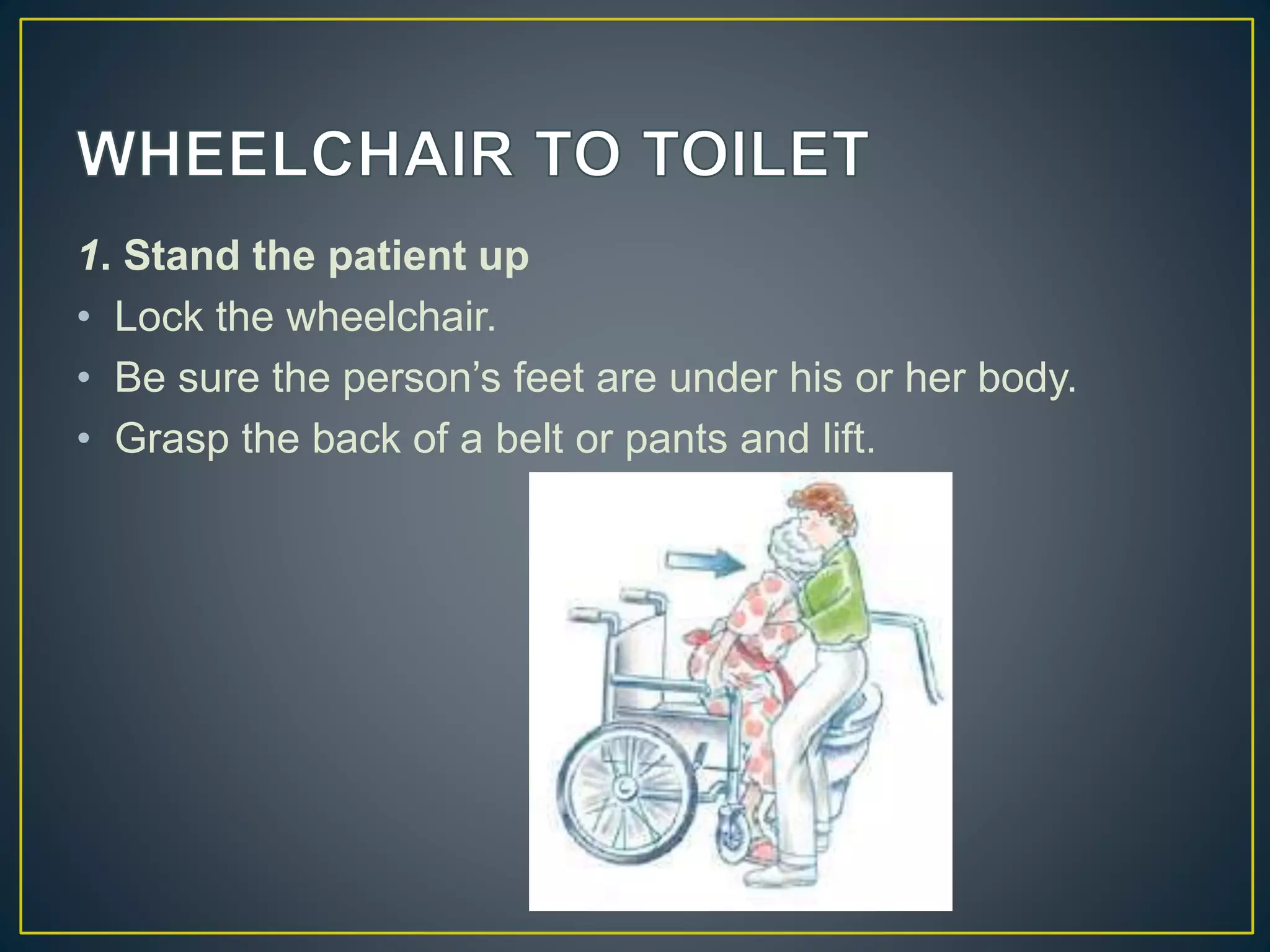
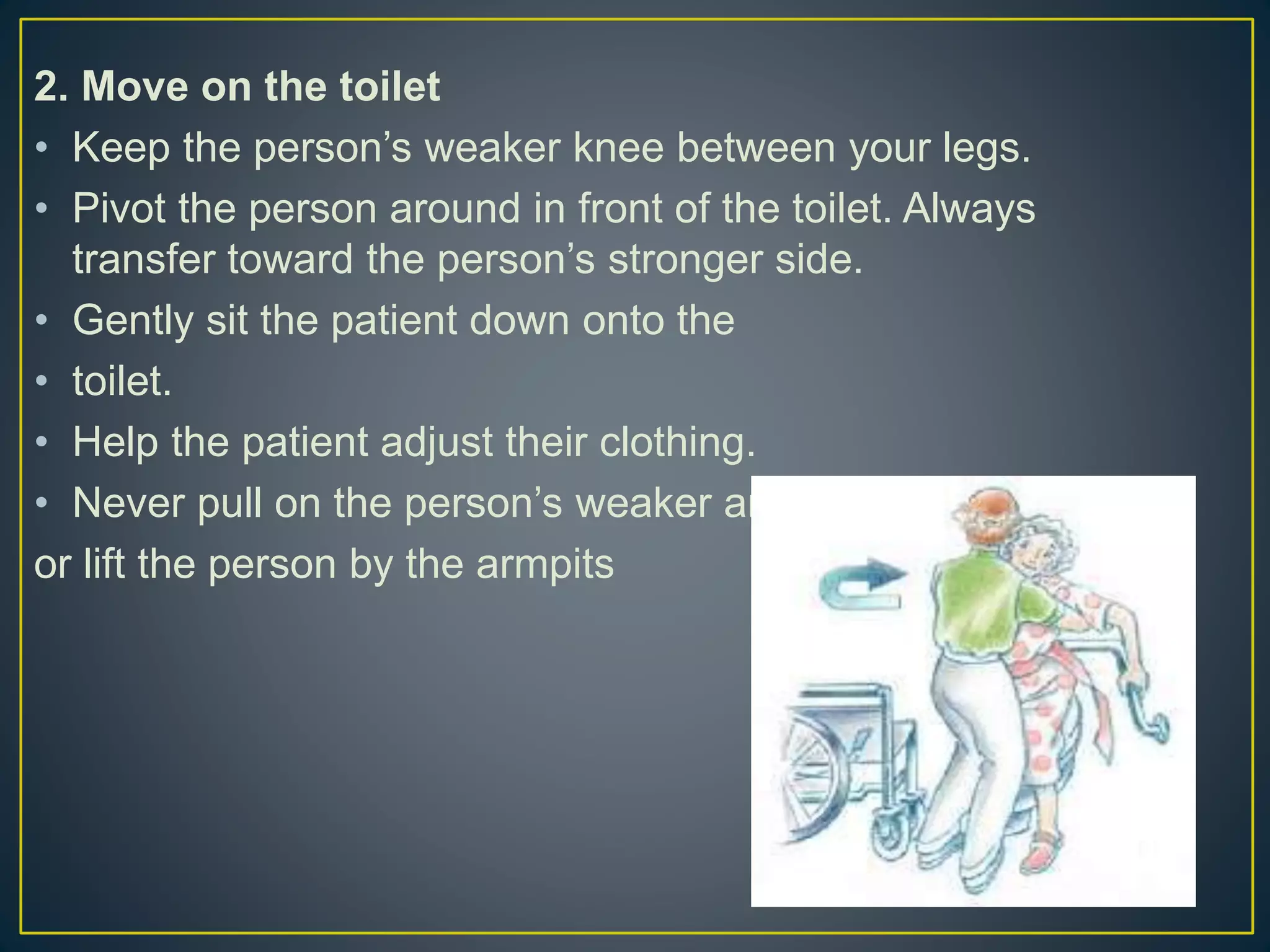
2) Common transfer techniques include dependent, assisted, and independent transfers using devices like draw sheets, sliders, and boards.
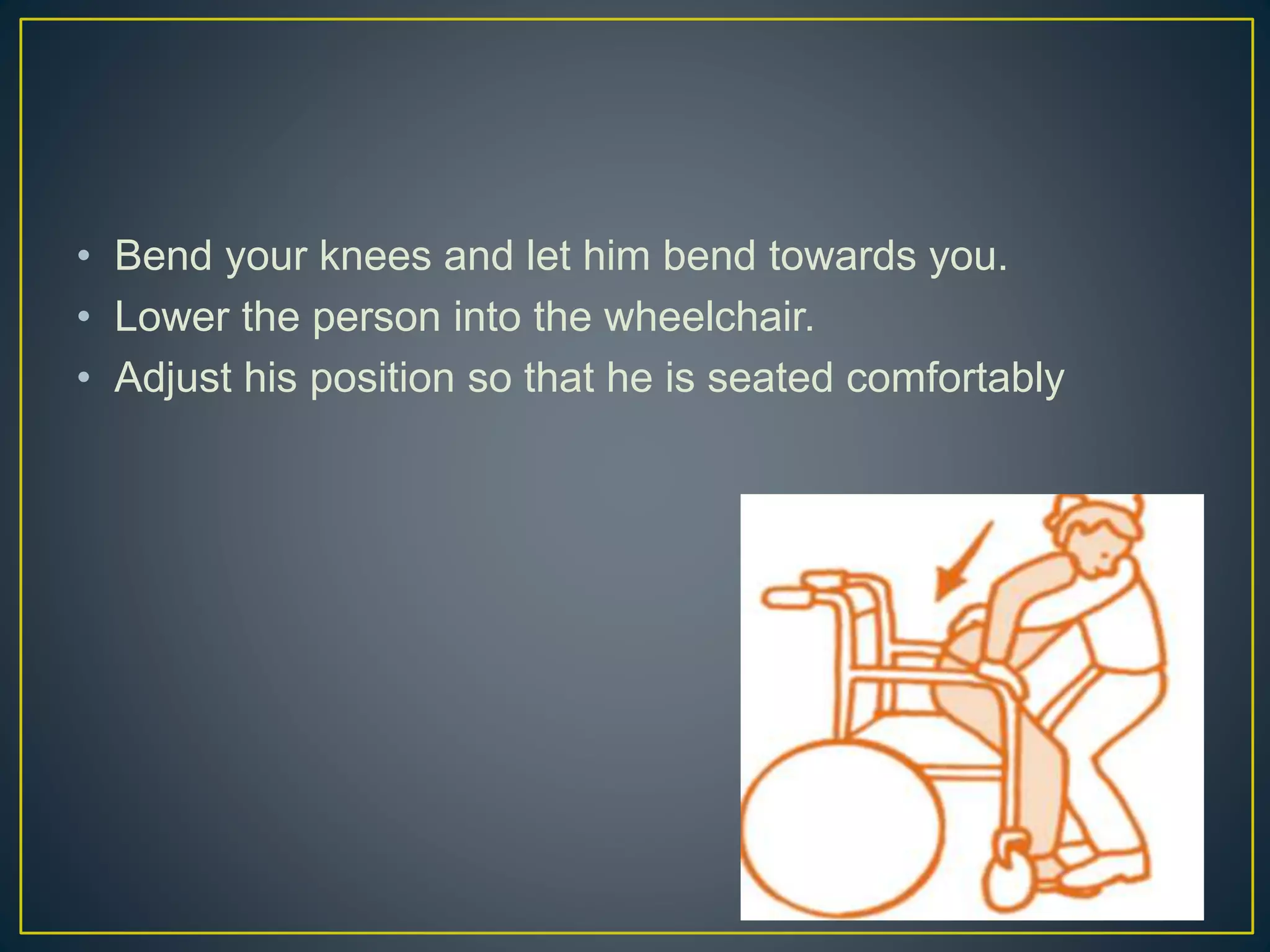
3) Proper body mechanics and communication are essential to avoid injury for both the patient and caregiver. Bend knees, keep back straight, and get help for heavy transfers.