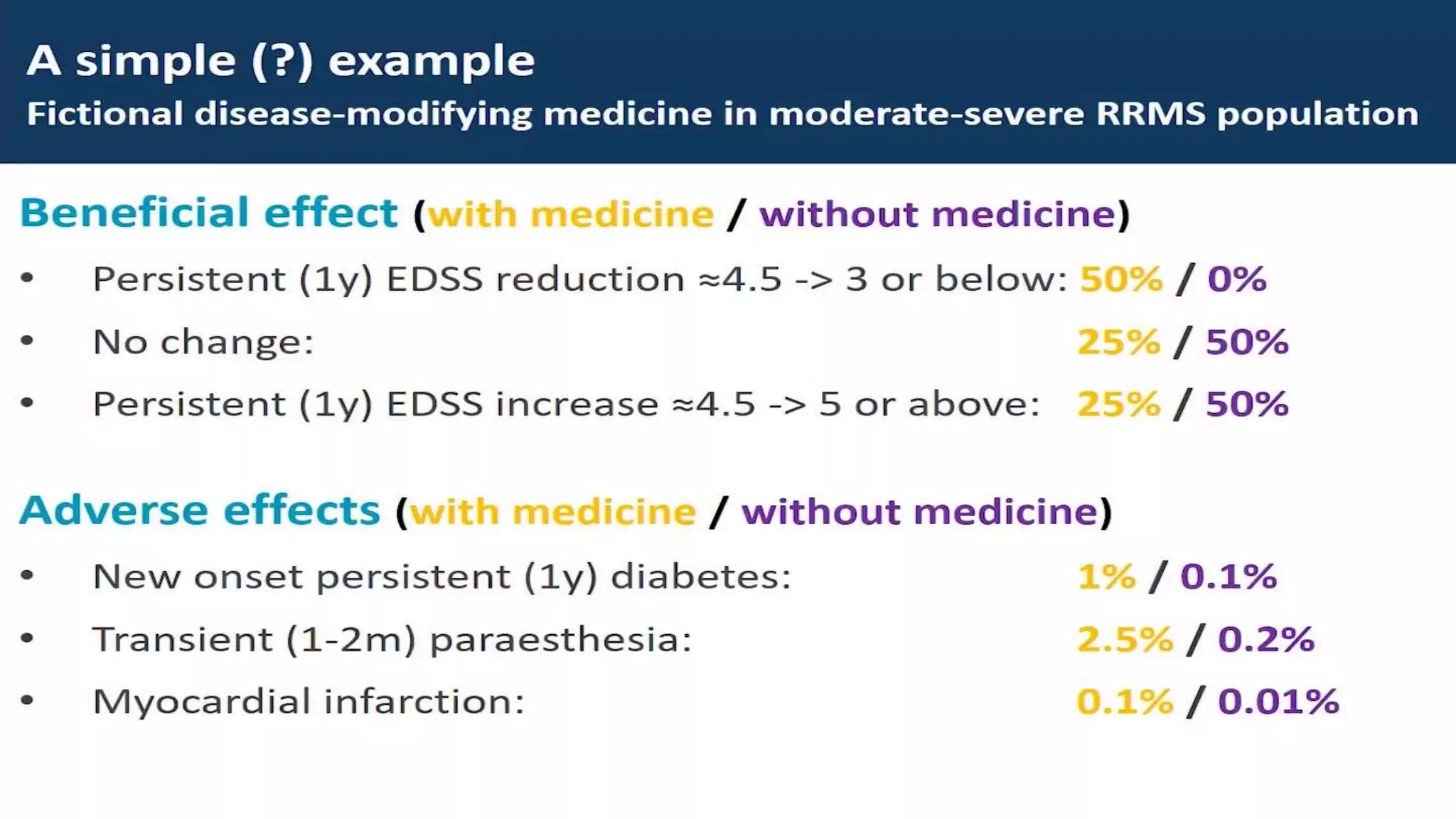
The document outlines the comprehensive evaluation of risk and benefit assessment in pharmacology, highlighting the types of risks (physical, psychological, social, economic) and potential benefits (physical, psychological, economic, societal). It emphasizes the importance of continuously assessing the risk-benefit ratio throughout the drug development lifecycle and mentions various methods and categories for risk evaluation. Additionally, it discusses the evolution of regulatory guidance on benefit-risk evaluation, showcasing the dynamic nature of this process.