Downloaded 11 times

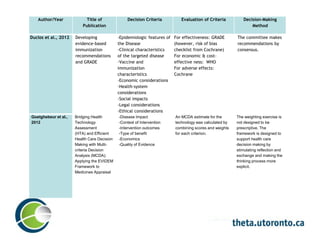
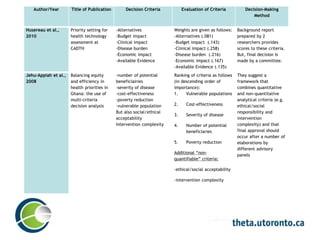
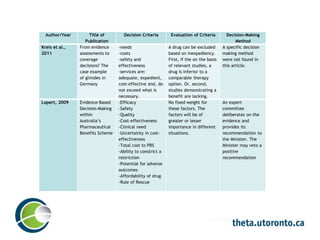

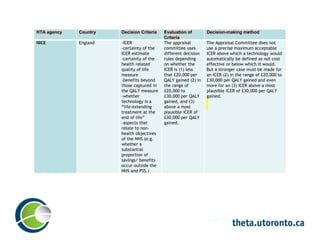
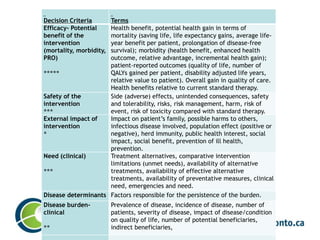
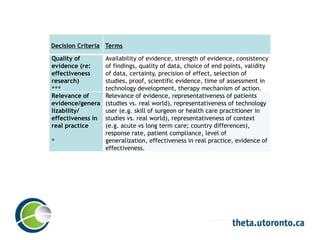

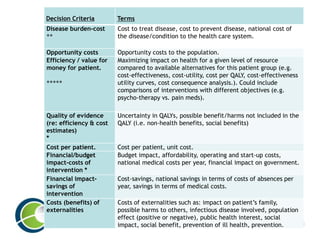
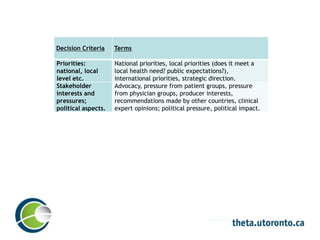
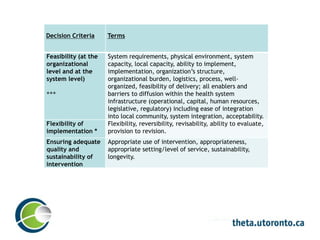

The document summarizes a literature review examining decision-making methodologies used in health technology appraisal processes. It describes common decision criteria identified in the literature, including efficacy, safety, disease burden, quality of evidence, ethics and cost-effectiveness. Decision-making methods reviewed integrate these criteria through approaches like assigning weights, ranking criteria or using decision rules. The literature search included publications from organizations in several countries.




















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

