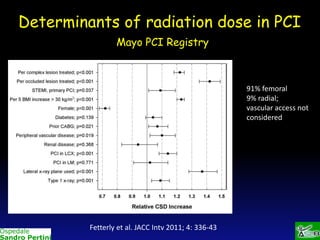
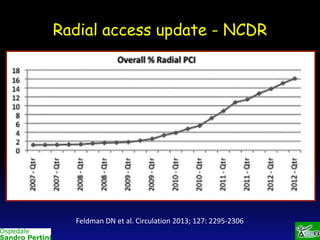
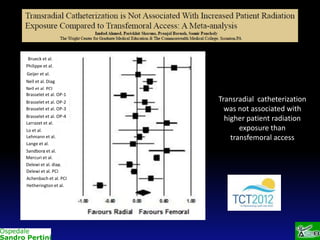
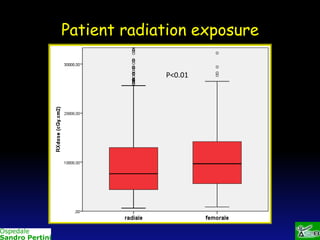
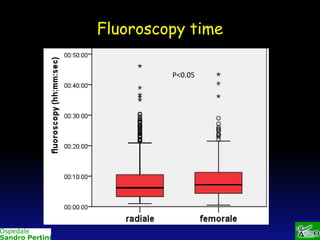
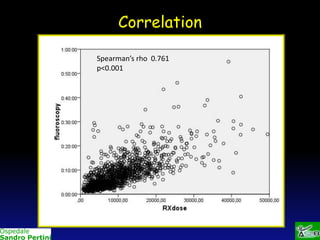
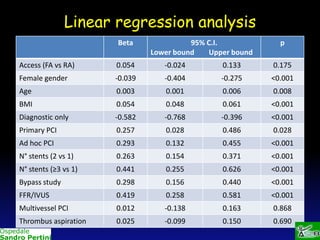
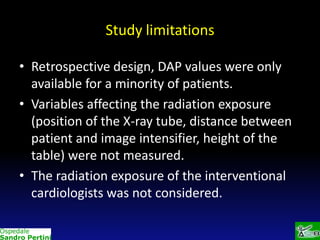
This study compares radiation exposure during percutaneous coronary interventions using radial versus femoral access. It found no significant difference in patient radiation exposure between the two approaches after adjusting for confounders, with a predominance of radial access procedures. Limitations include its retrospective design and limited DAP data availability.