


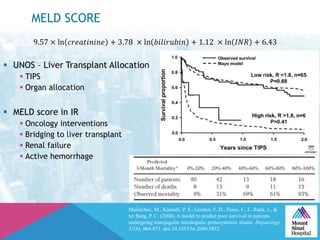
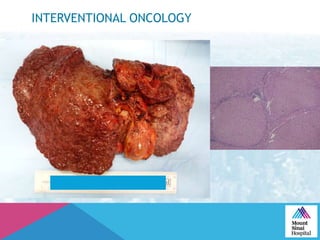

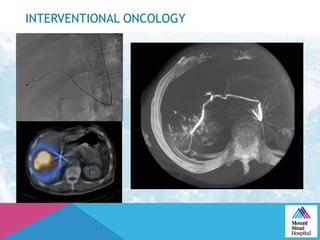
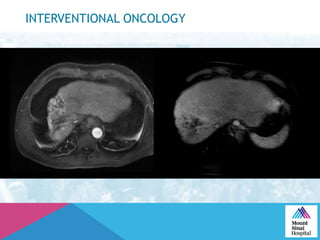
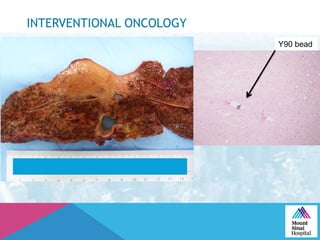

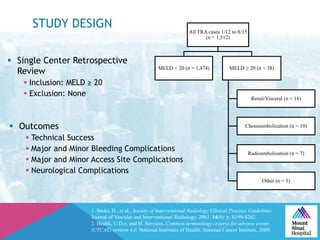
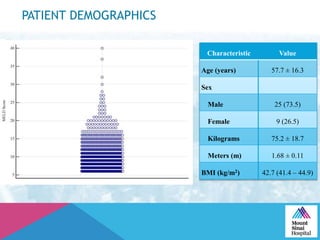

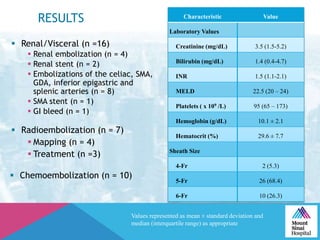

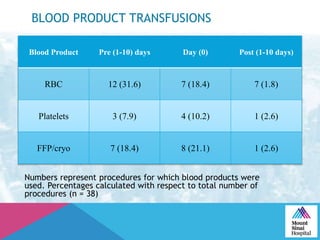
This document summarizes a study examining the use of transradial access (TRA) for non-coronary interventions in patients with severe hepatic dysfunction (MELD score ≥ 20). The study found TRA to be feasible in this high-risk population with a 100% technical success rate and very low rates of bleeding (0%) and access site (1 minor hematoma) complications. TRA in patients with liver dysfunction was shown to be safe and effective for renal/visceral interventions like embolization and stenting as well as radioembolization procedures, with few coagulation blood products required.


































































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)








