
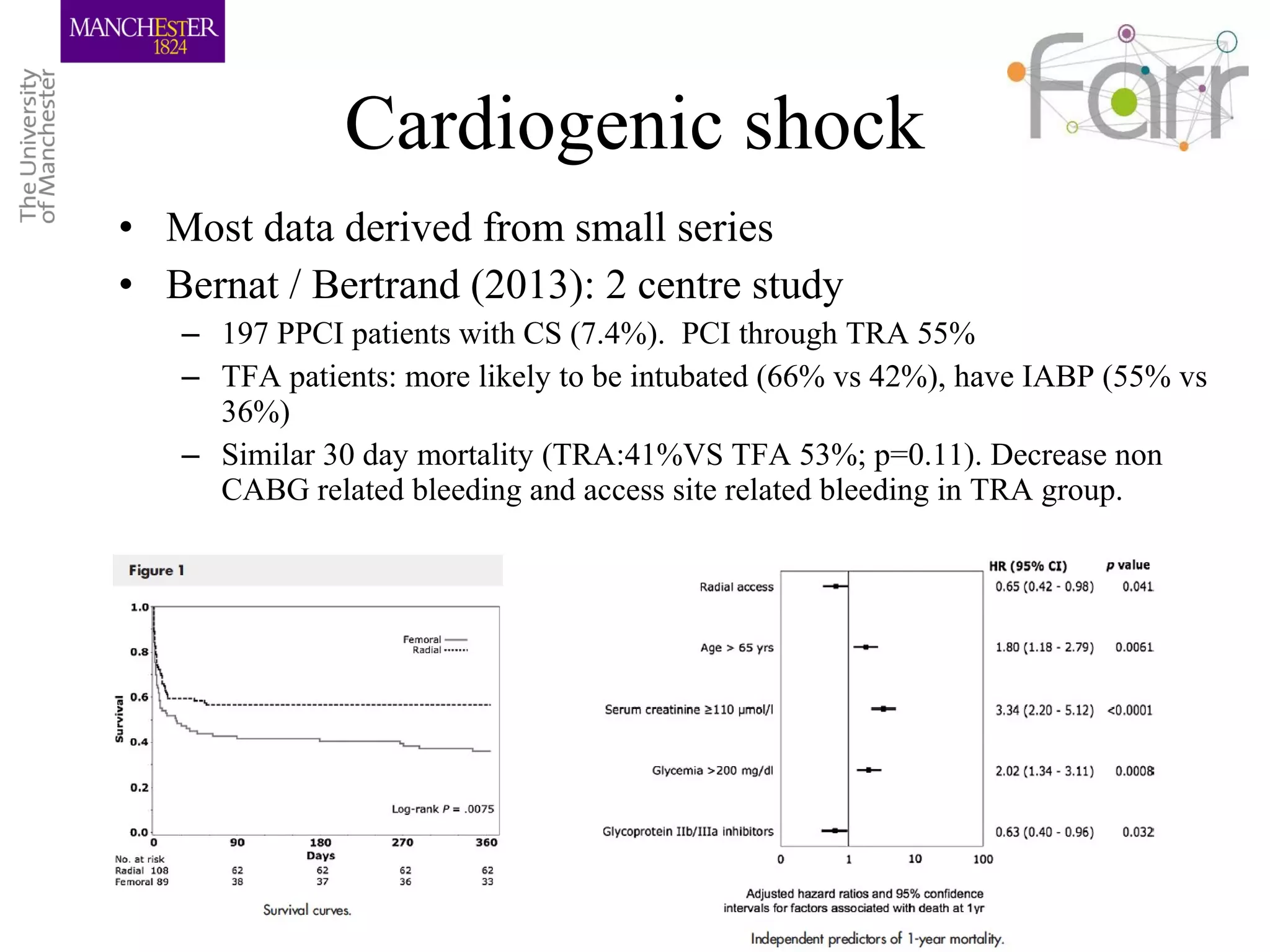
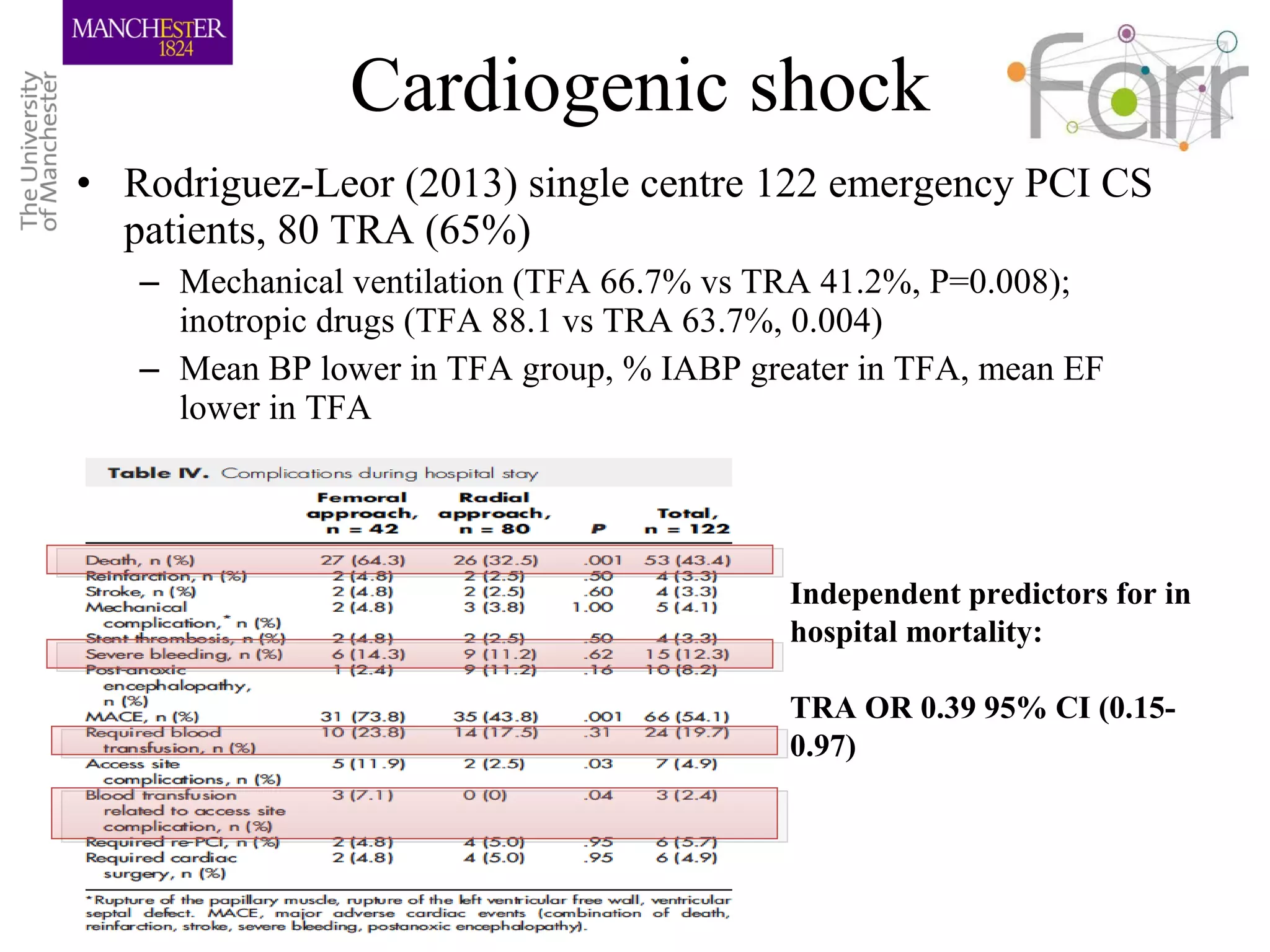
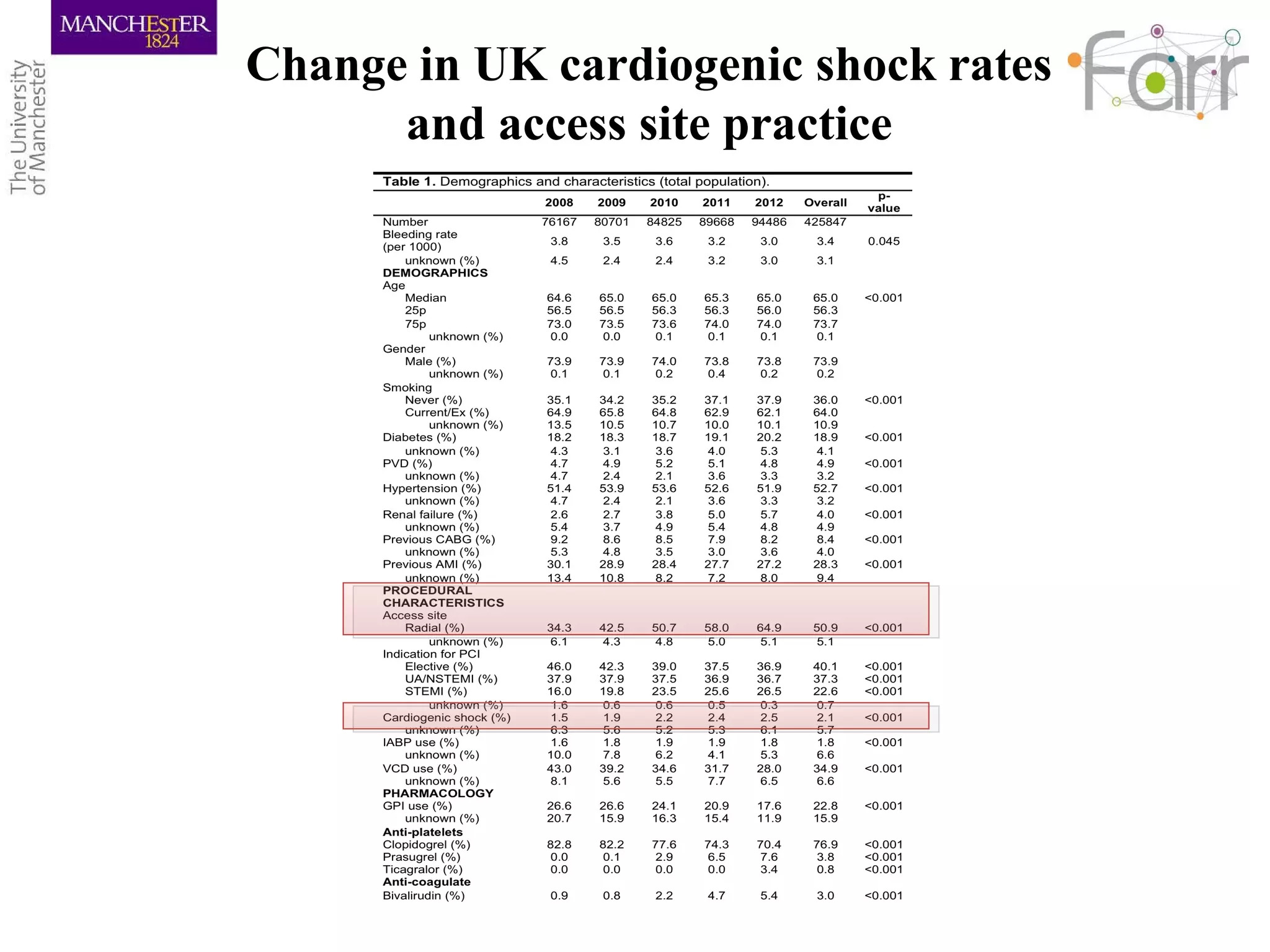
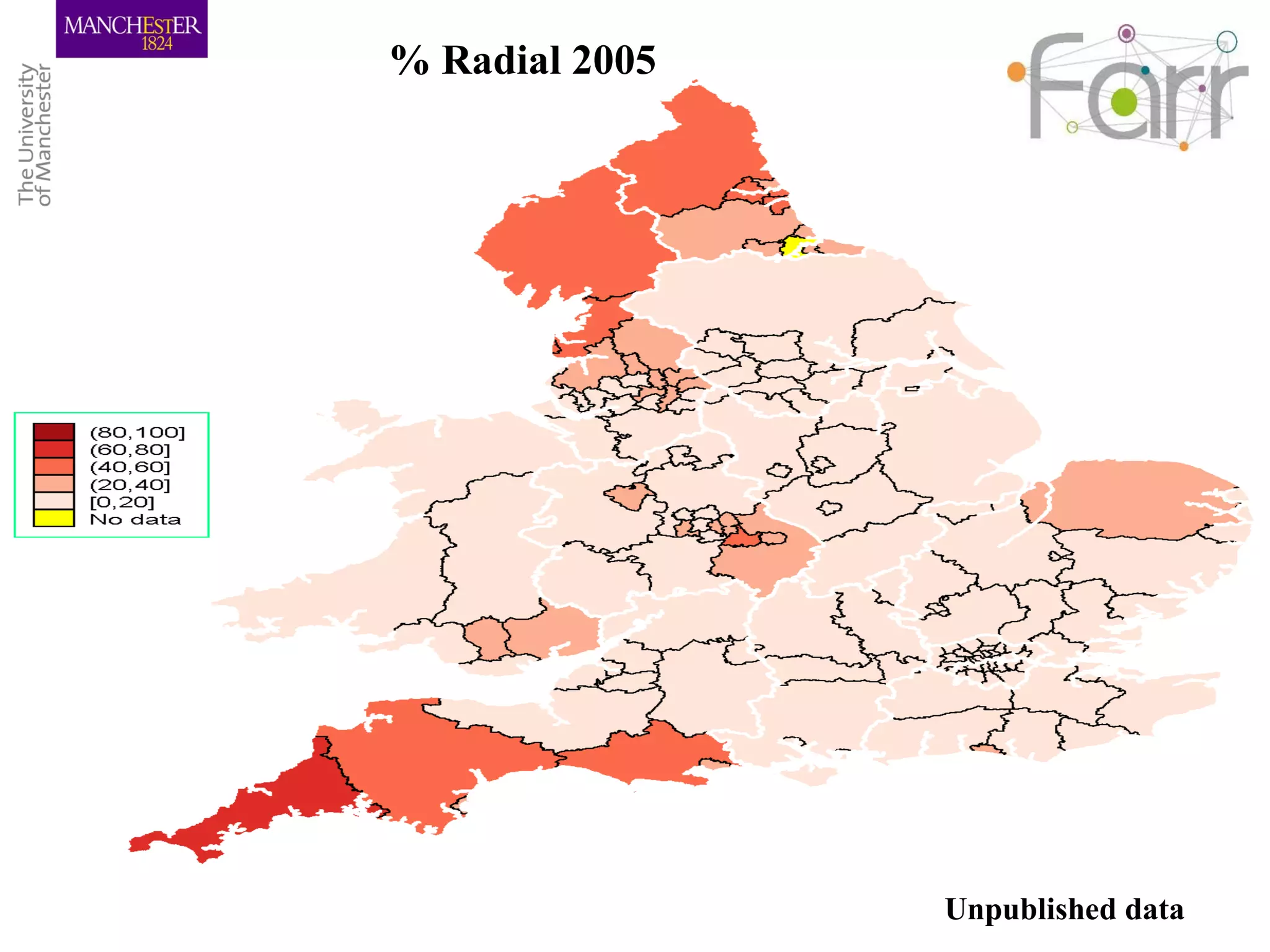
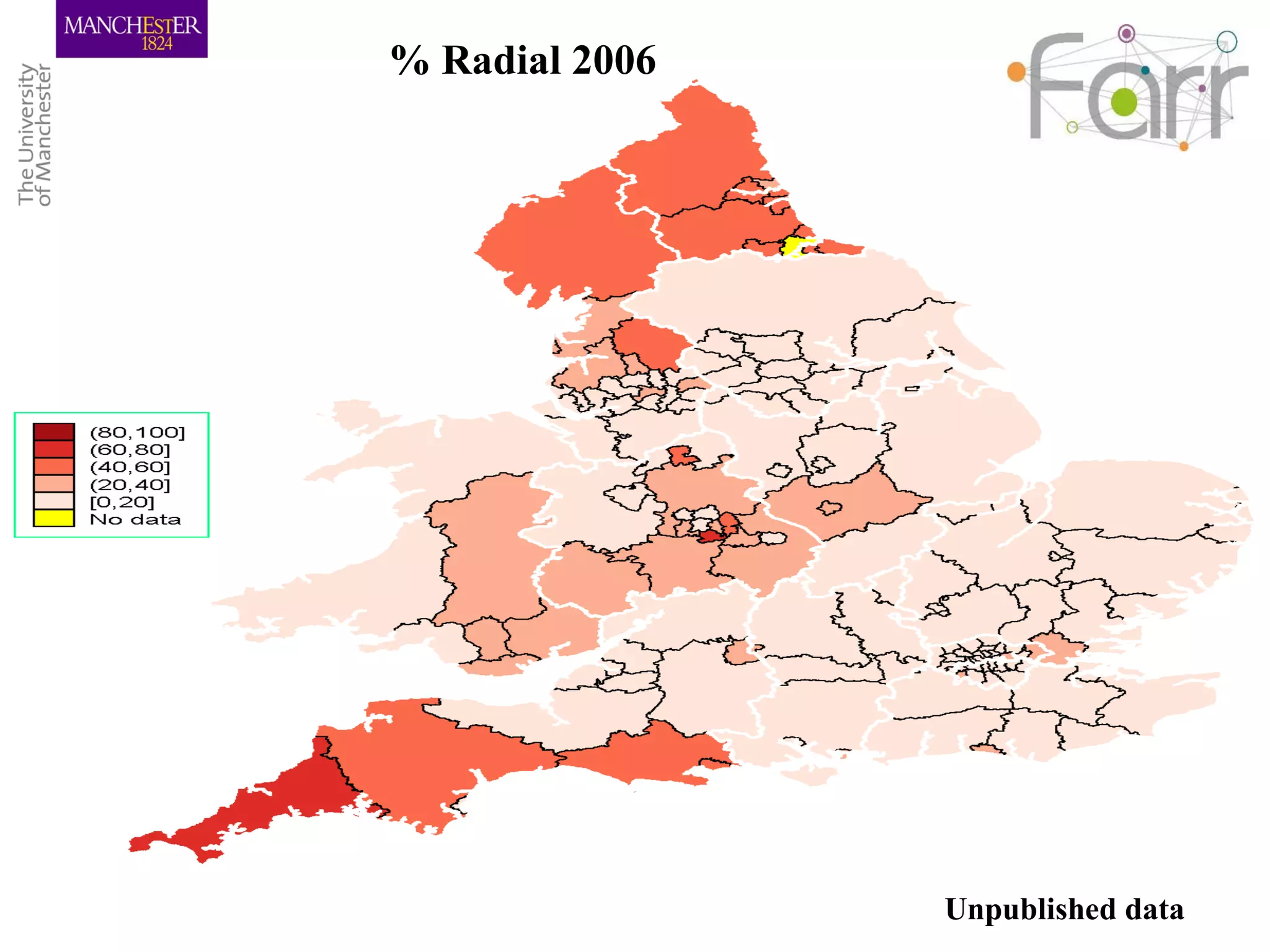
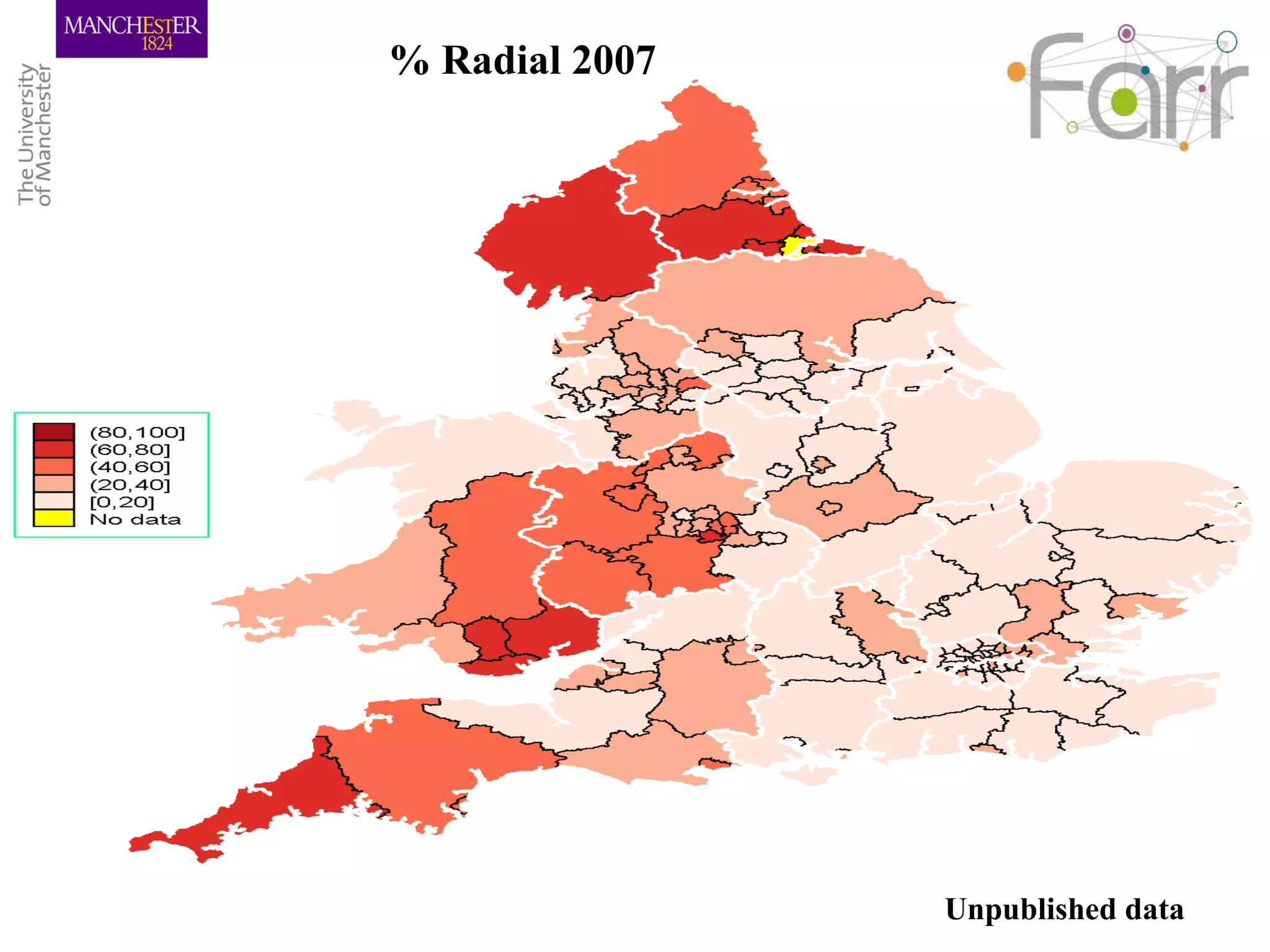
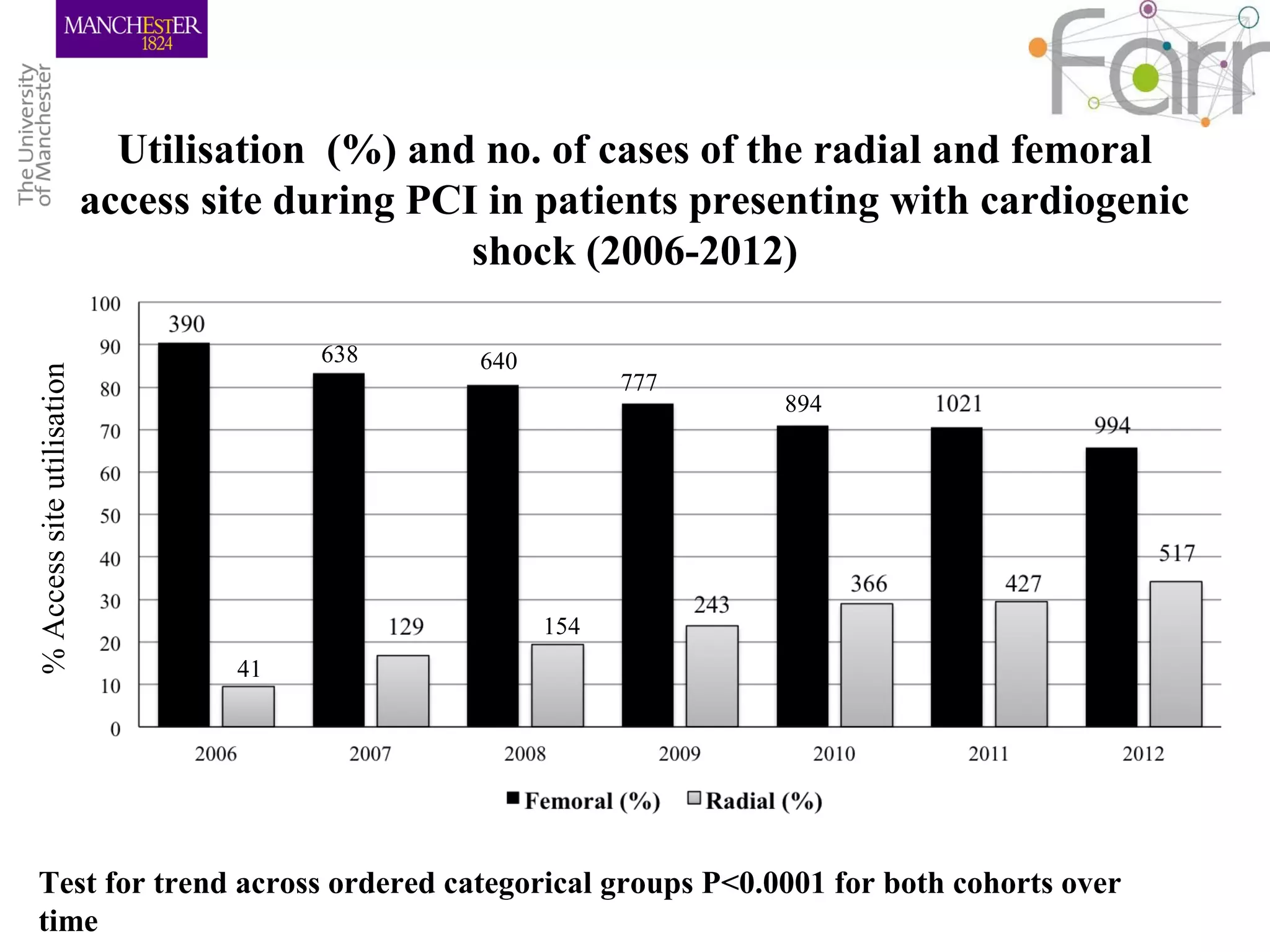
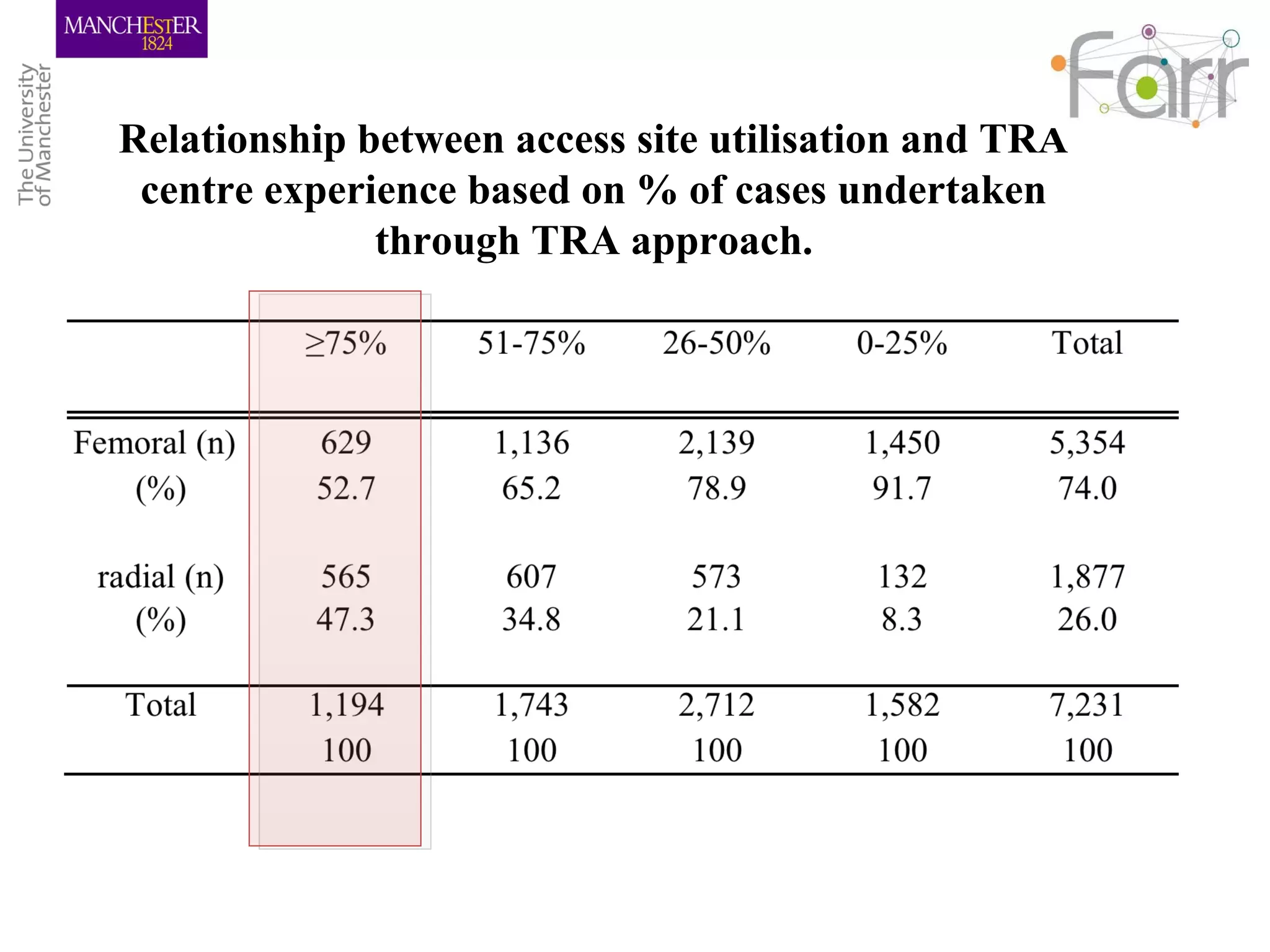
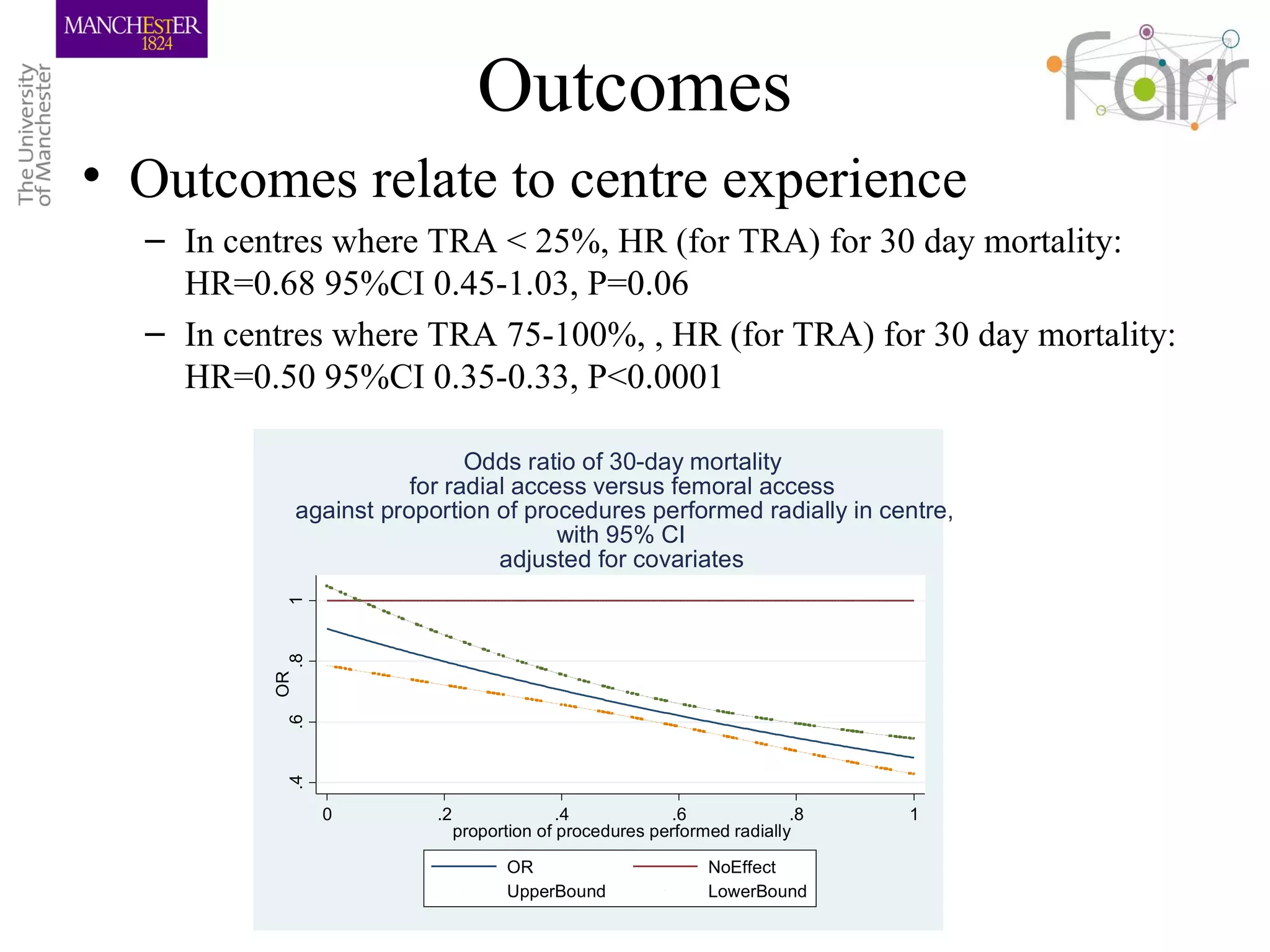
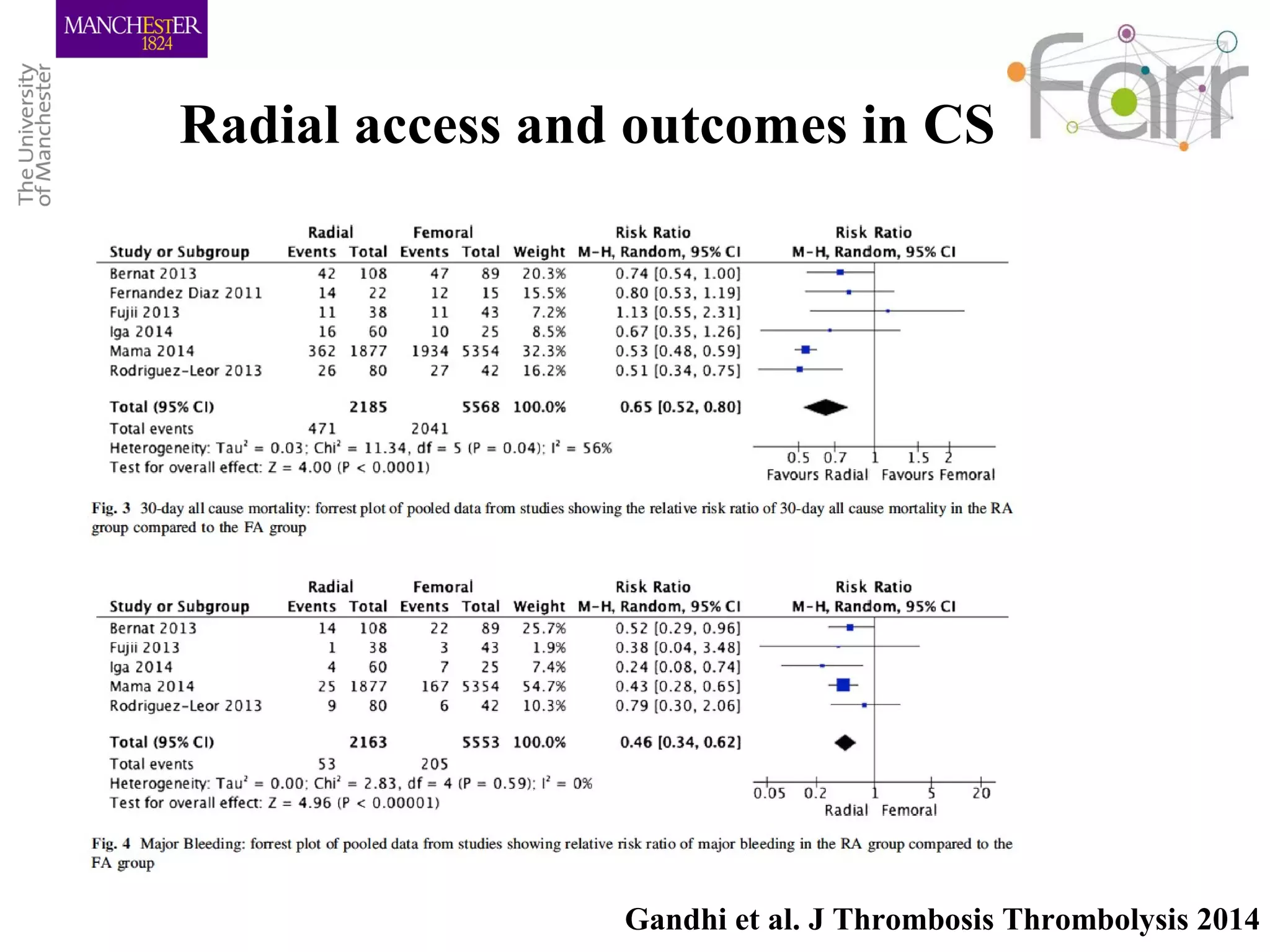
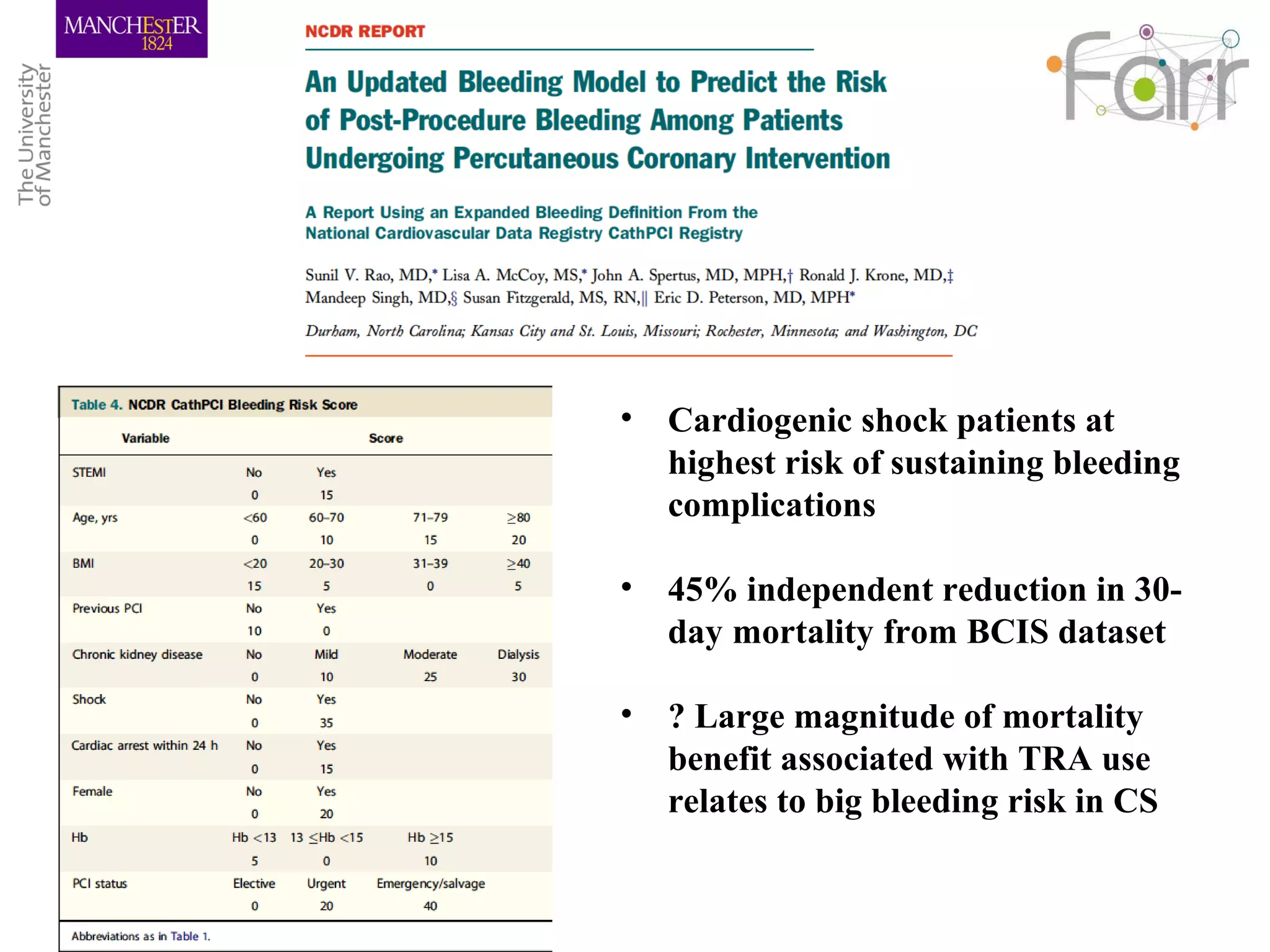
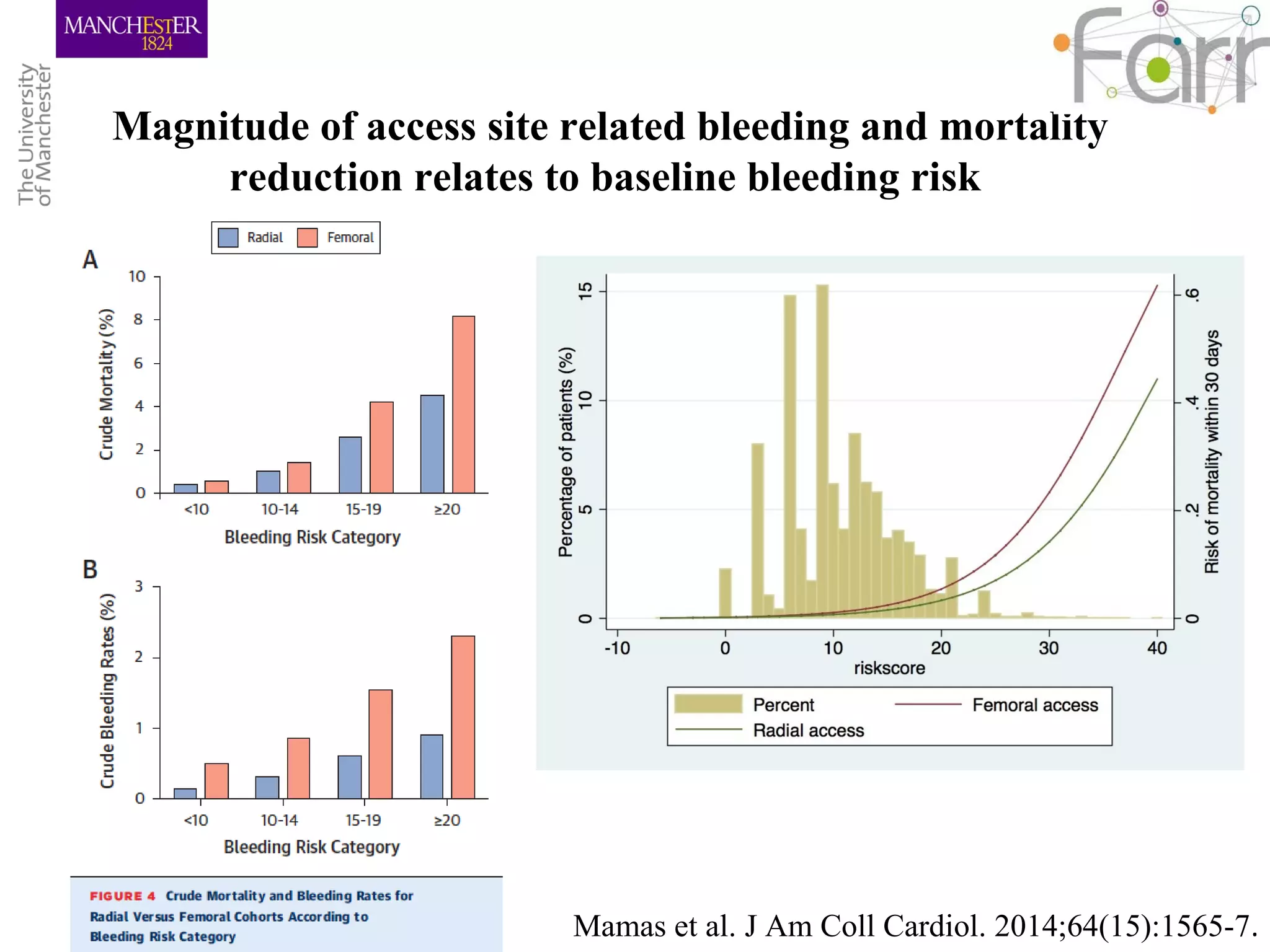
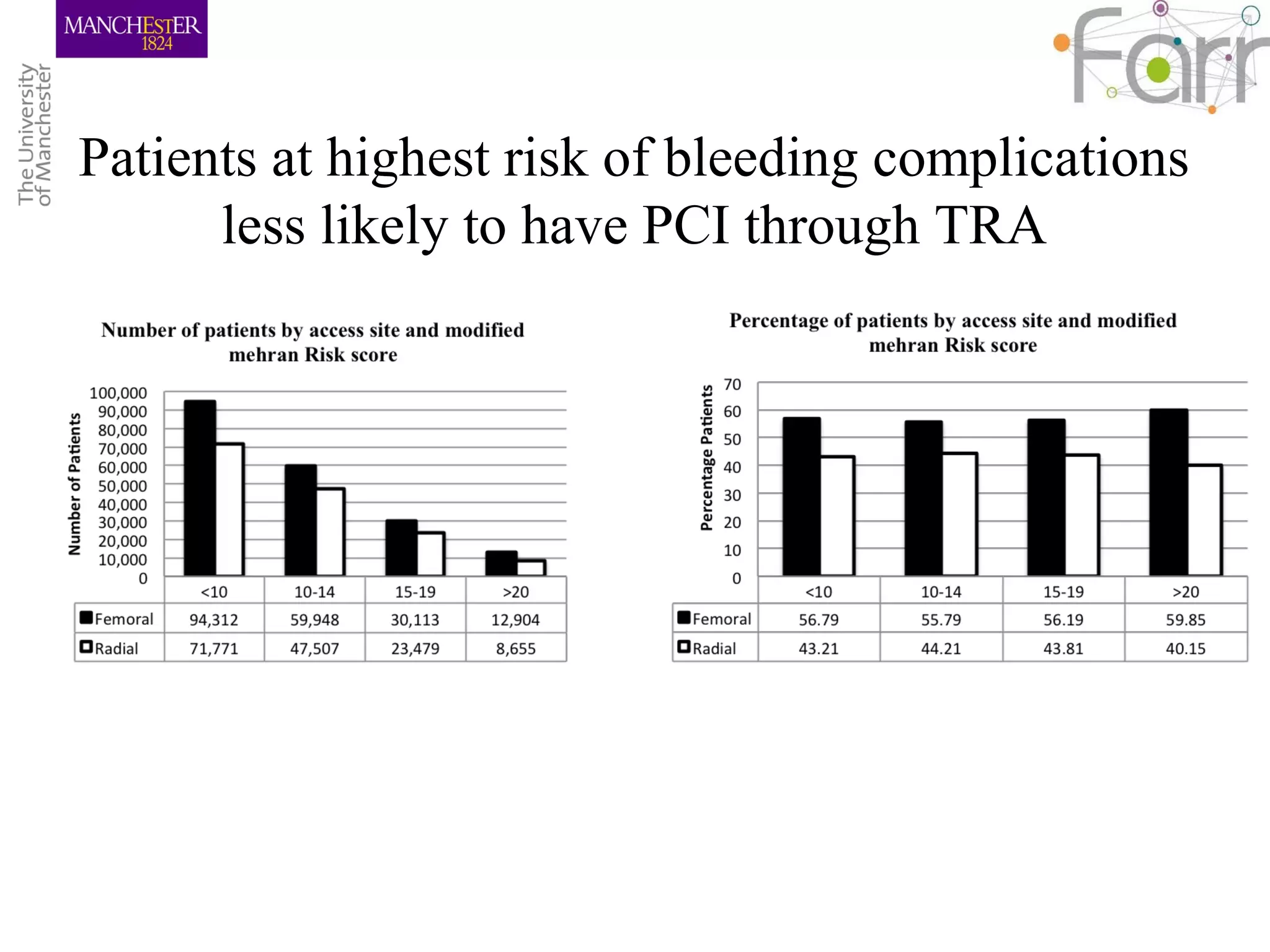
Cardiogenic shock is a leading cause of death in AMI patients, with mortality rates between 30-60%. While radial access has been shown to reduce bleeding complications, patients presenting with cardiogenic shock are often treated via transfemoral access. Recent studies have demonstrated that radial access PCI is feasible in cardiogenic shock patients, with one study showing a reduction in in-hospital mortality for radial versus transfemoral access. However, experienced radial centers only use the radial approach in around 50% of cardiogenic shock cases, indicating radial access is still underutilized despite potential benefits in this high-risk group.











































































































