
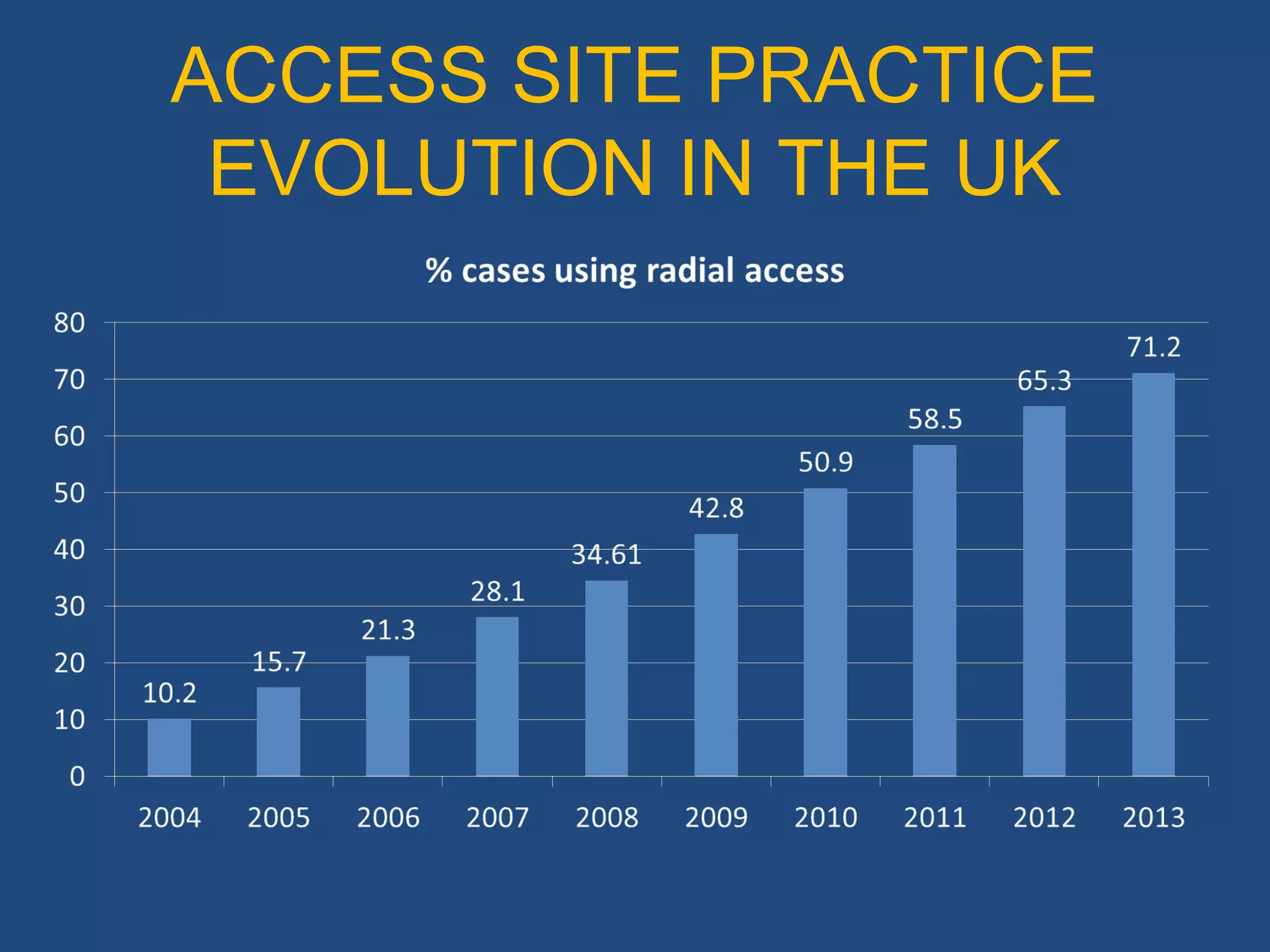
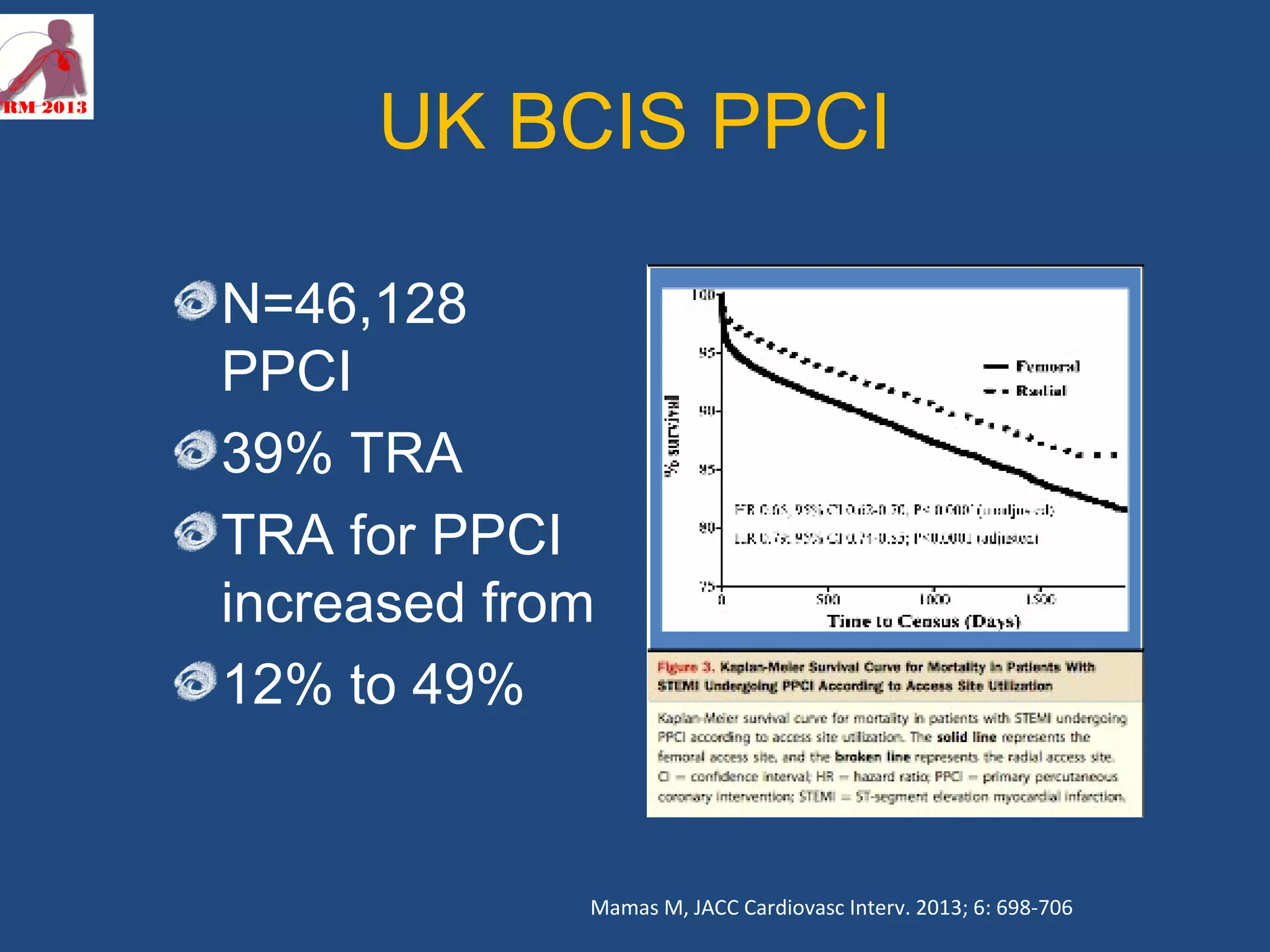
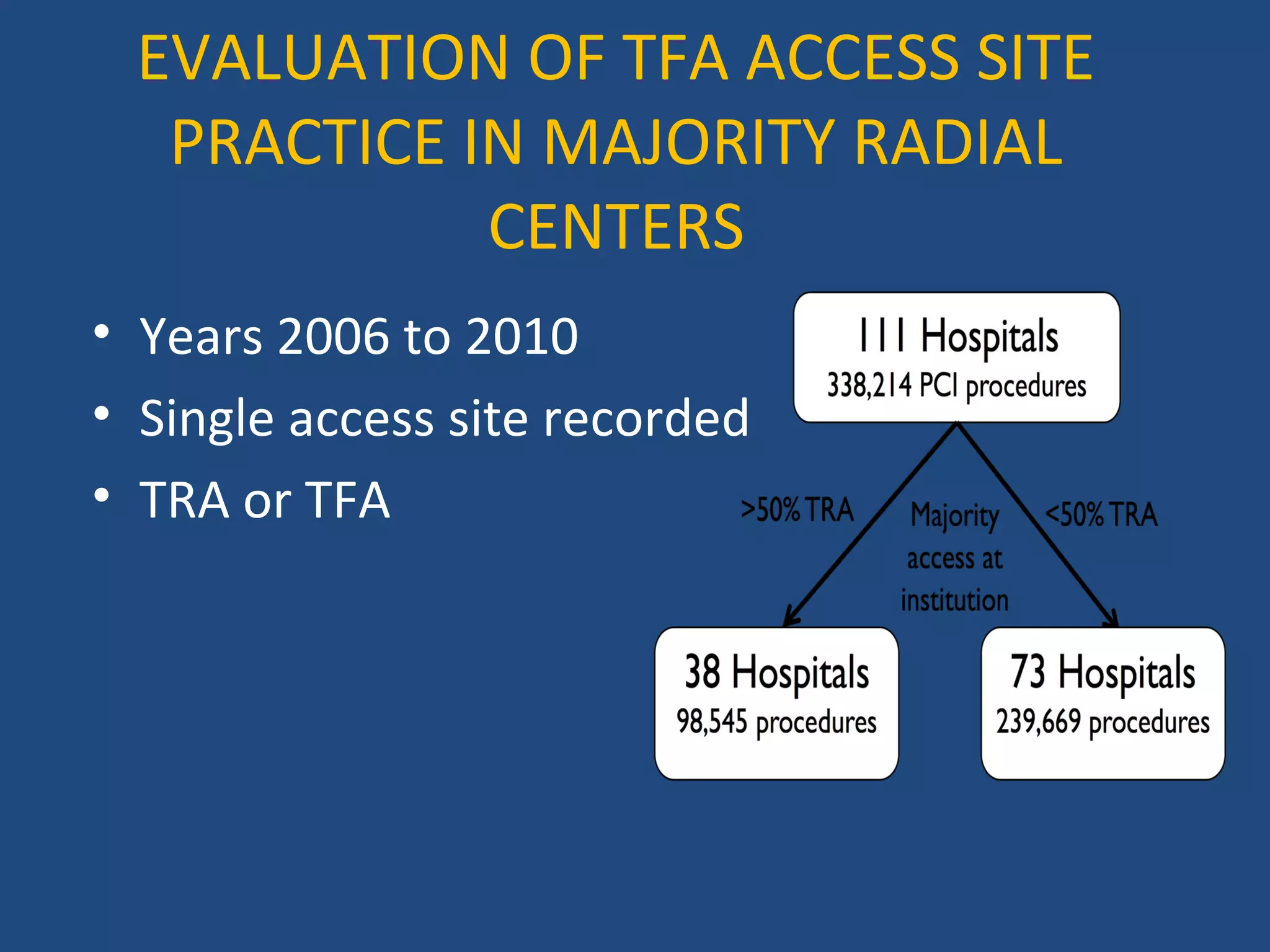
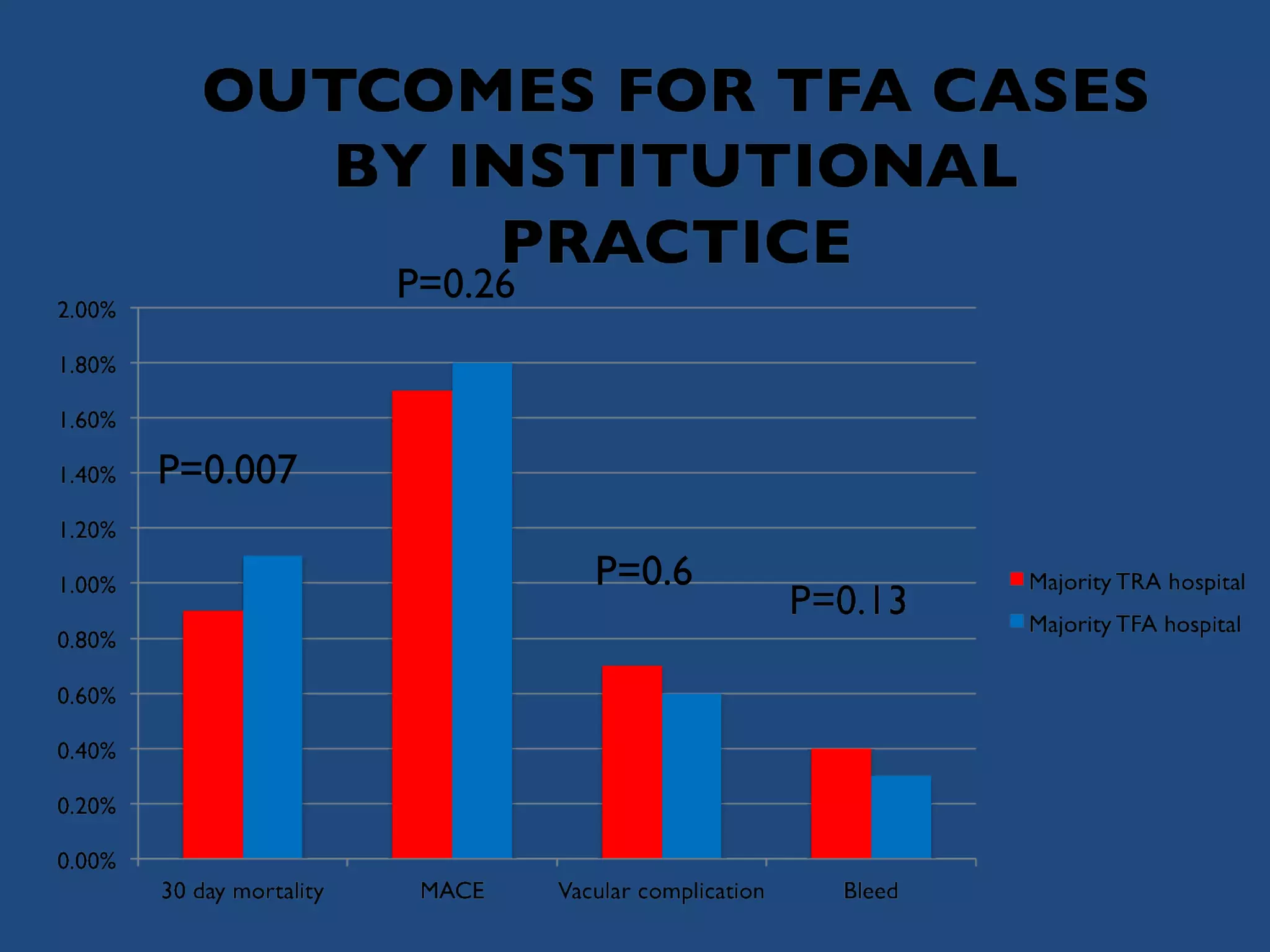
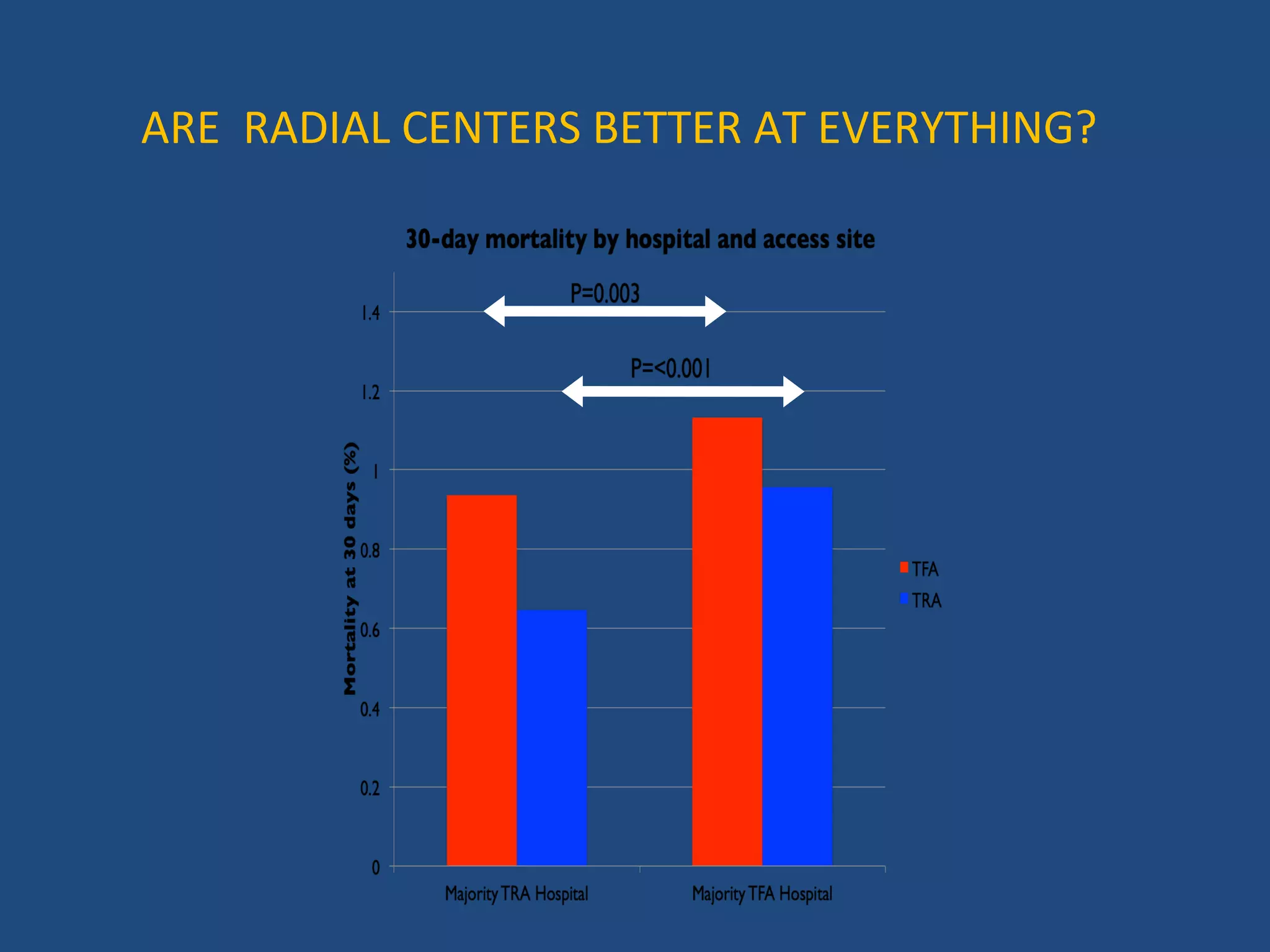
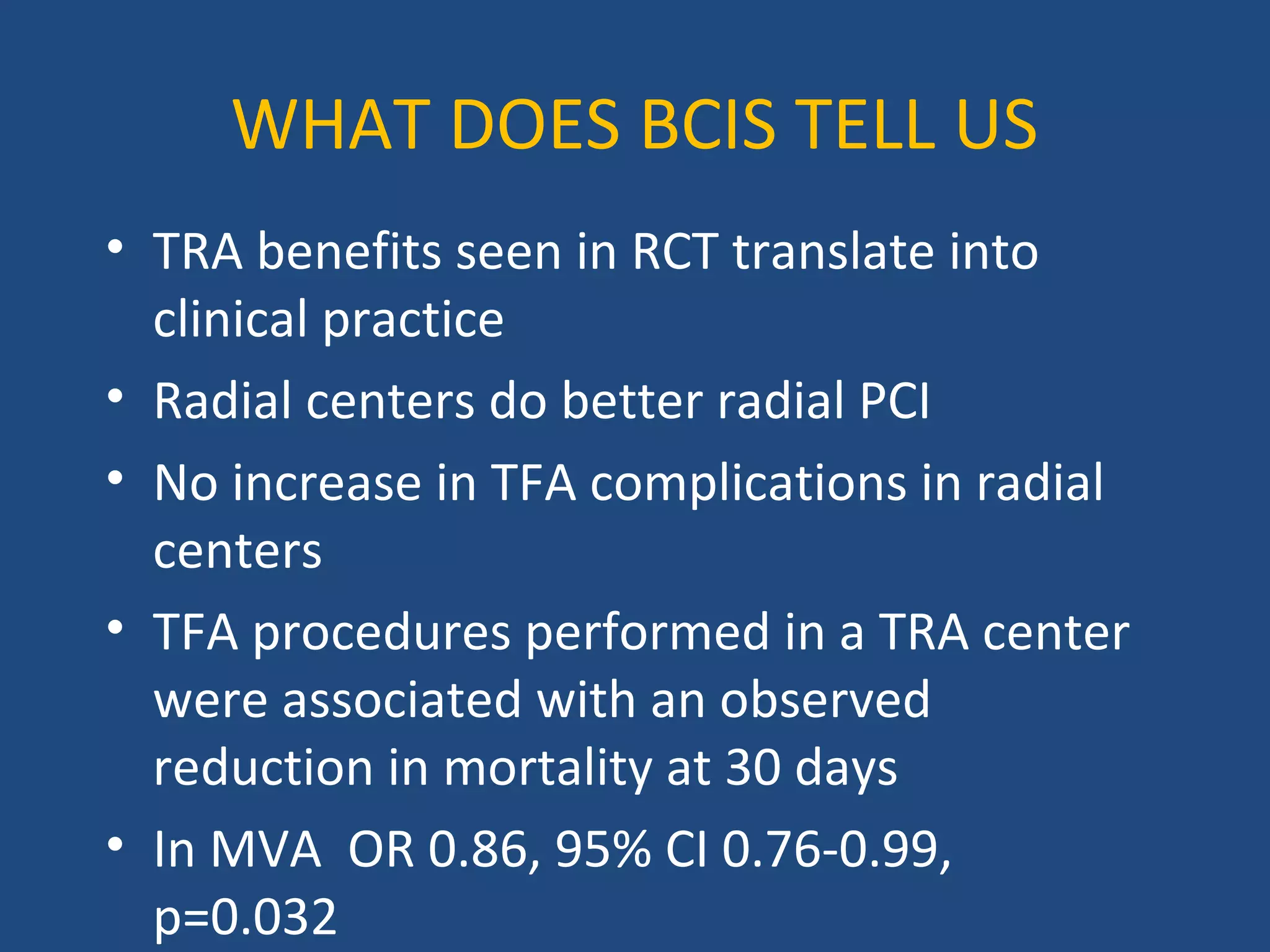
- A study of 1352 PCI procedures at a radial center found that while 25.2% used femoral access, these cases had fewer complications (12.5% hematomas vs 6.25% requiring intervention) than expected given reduced femoral experience. - Analysis of UK PCI data found radial use increased from 12-49% for PPCI, with no increase in femoral complications at radial centers and a possible reduction in 30-day mortality for femoral cases at radial centers. - While radial access is safer, some patients still require femoral, and data suggests radial operators have good outcomes for these cases as well.























































































