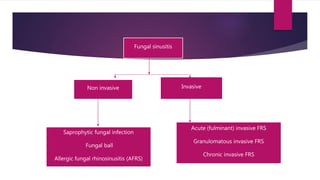
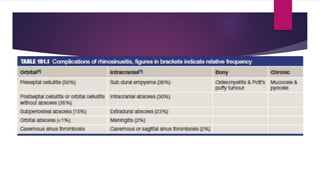
This document discusses various types of fungal sinusitis. It begins by categorizing fungal rhinosinusitis into invasive and non-invasive types based on the presence or absence of fungal invasion of tissue. It then describes the different subtypes of non-invasive and invasive fungal sinusitis in detail, including their pathogenesis, clinical presentation, diagnosis and management. It also discusses potential complications of fungal sinusitis such as orbital or intracranial infections that can arise from local or distant spread beyond the paranasal sinuses.