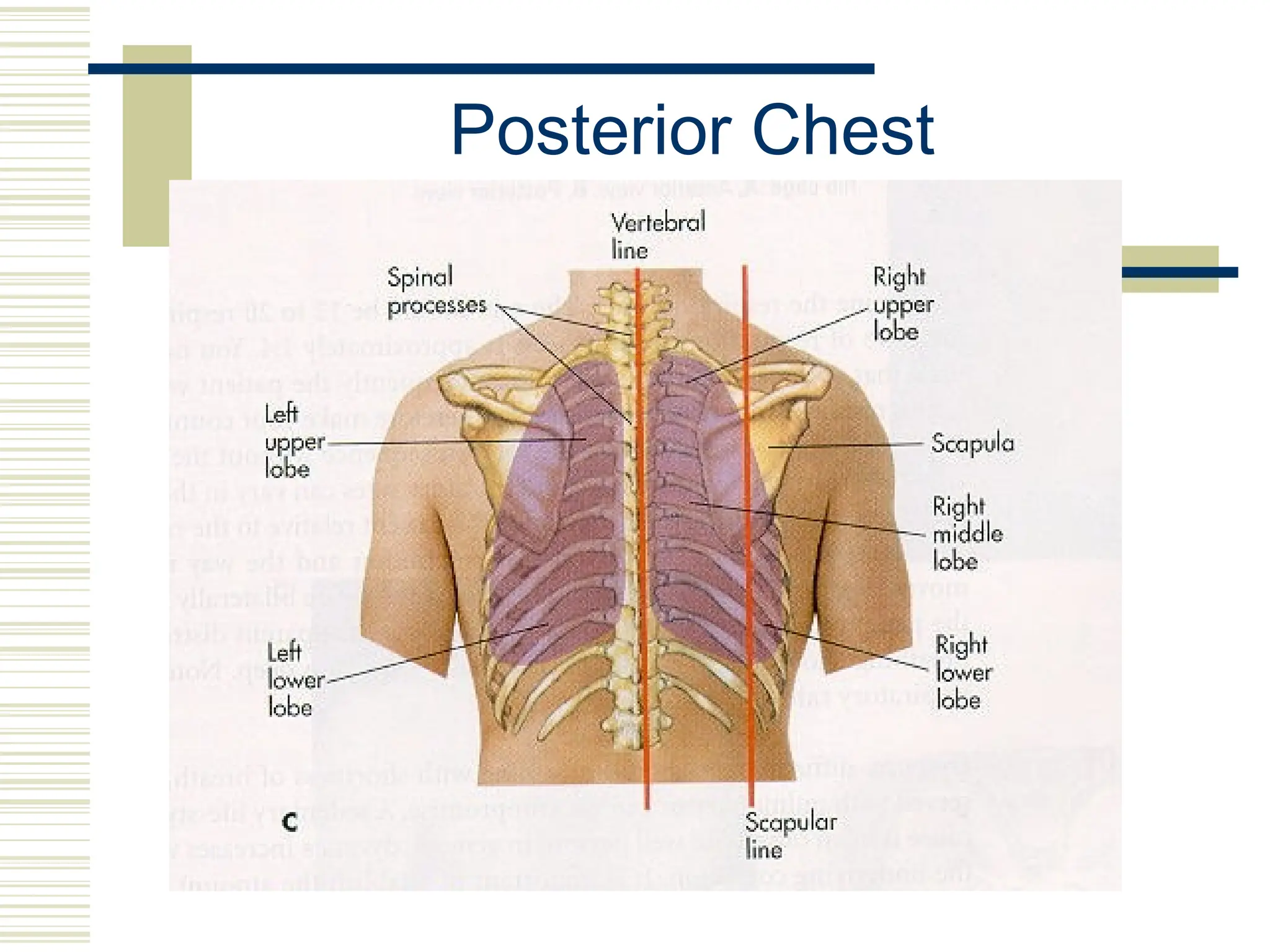
This document provides information on assessing the chest and lungs through physical examination. It discusses the relevant anatomy, history taking, and examination techniques including inspection, palpation, percussion, and auscultation of the chest. Examination points for different populations like neonates, infants, pregnant women, and older adults are also reviewed. The goal is to evaluate the lungs, breathing, and chest wall in a systematic manner.













































![chapter 4 Physical diagnosis [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/physicaldiagnosisautosaved-250416123318-d2df54aa-thumbnail.jpg?width=640&height=640&fit=bounds)









![Respiratory System PE-1 [Autosaved].ppttiteciex](https://cdn.slidesharecdn.com/ss_thumbnails/respiratorysystempe-1autosaved-250113170401-72d39633-thumbnail.jpg?width=640&height=640&fit=bounds)










































