Downloaded 206 times



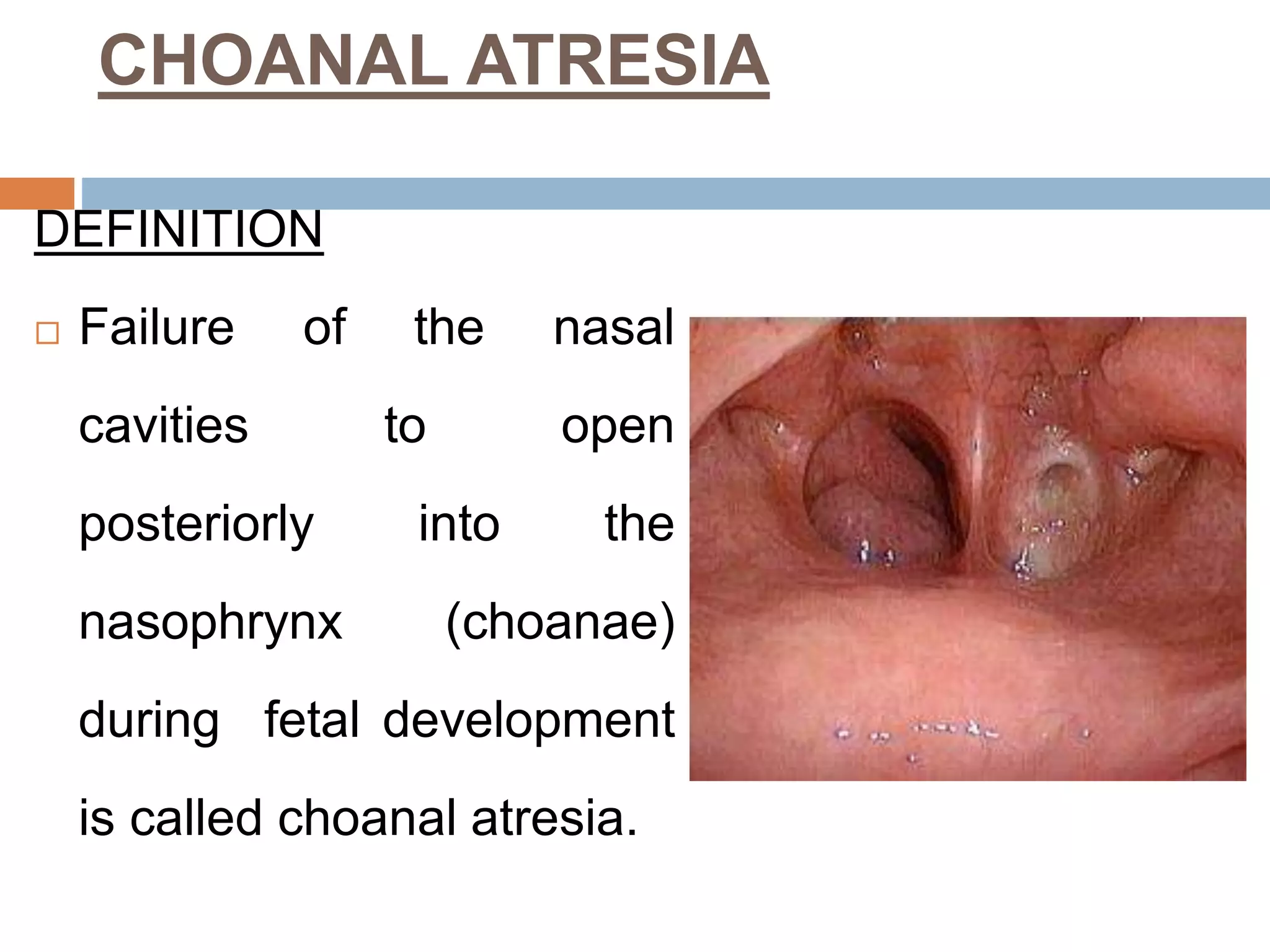



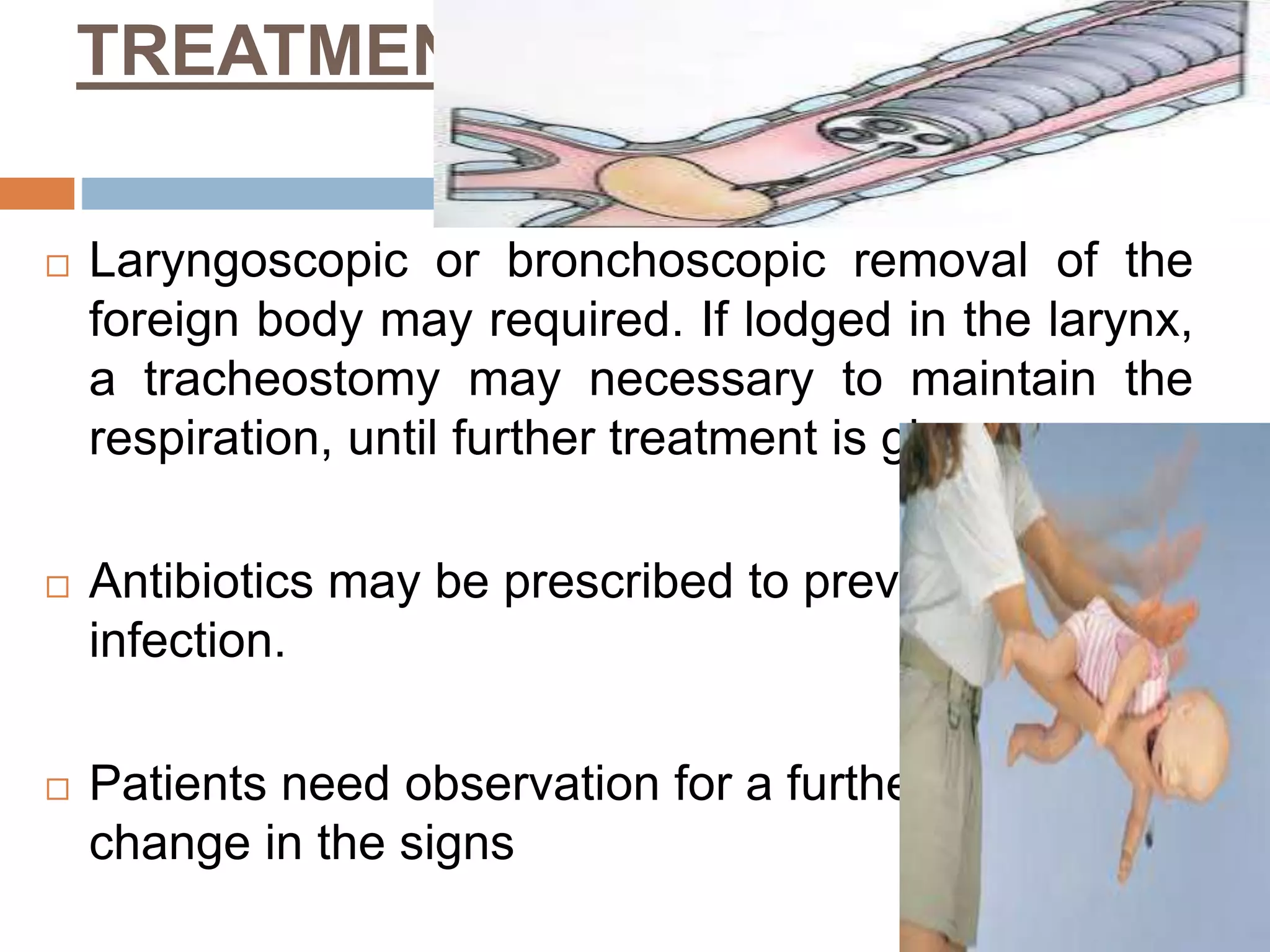
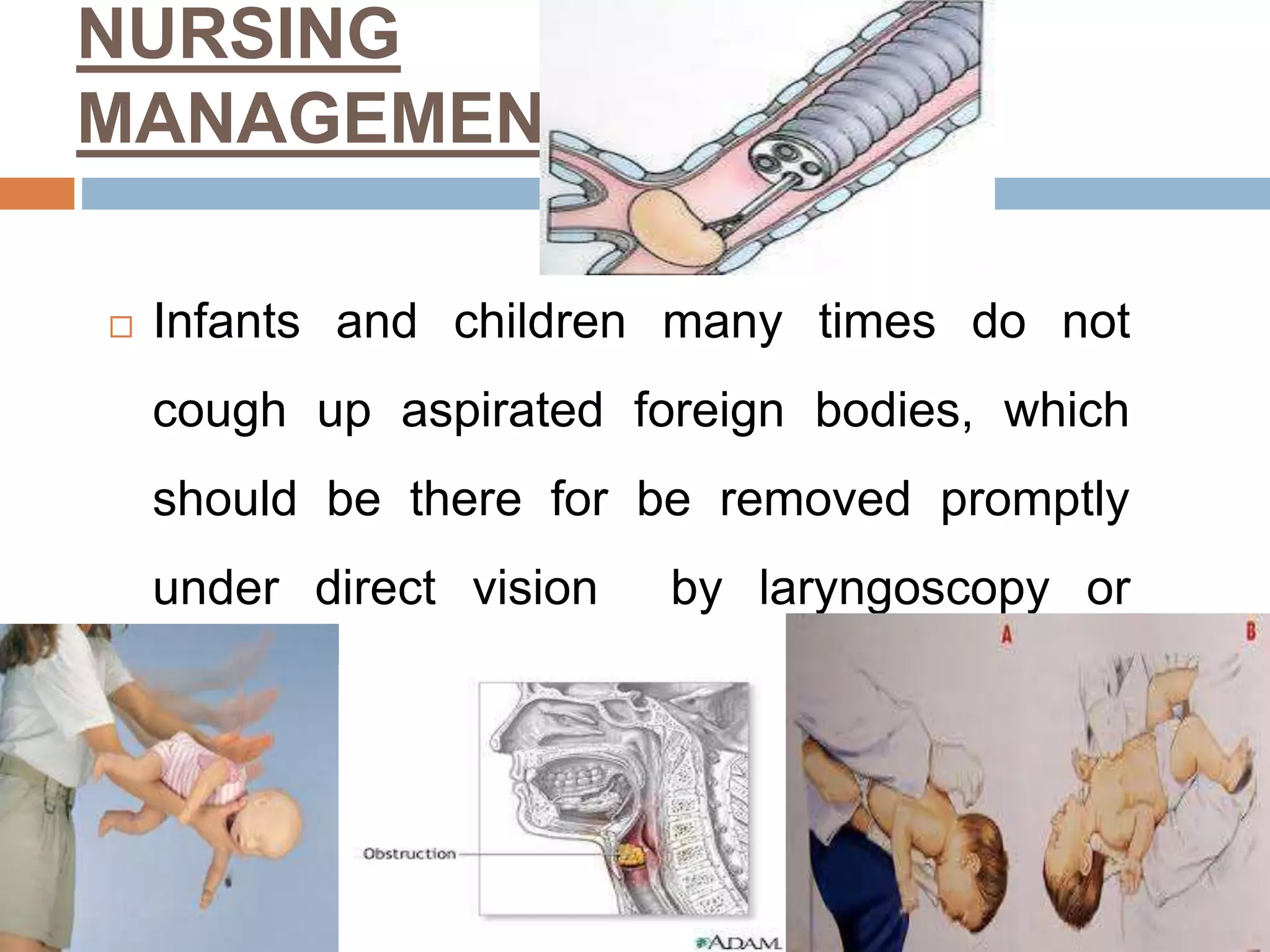


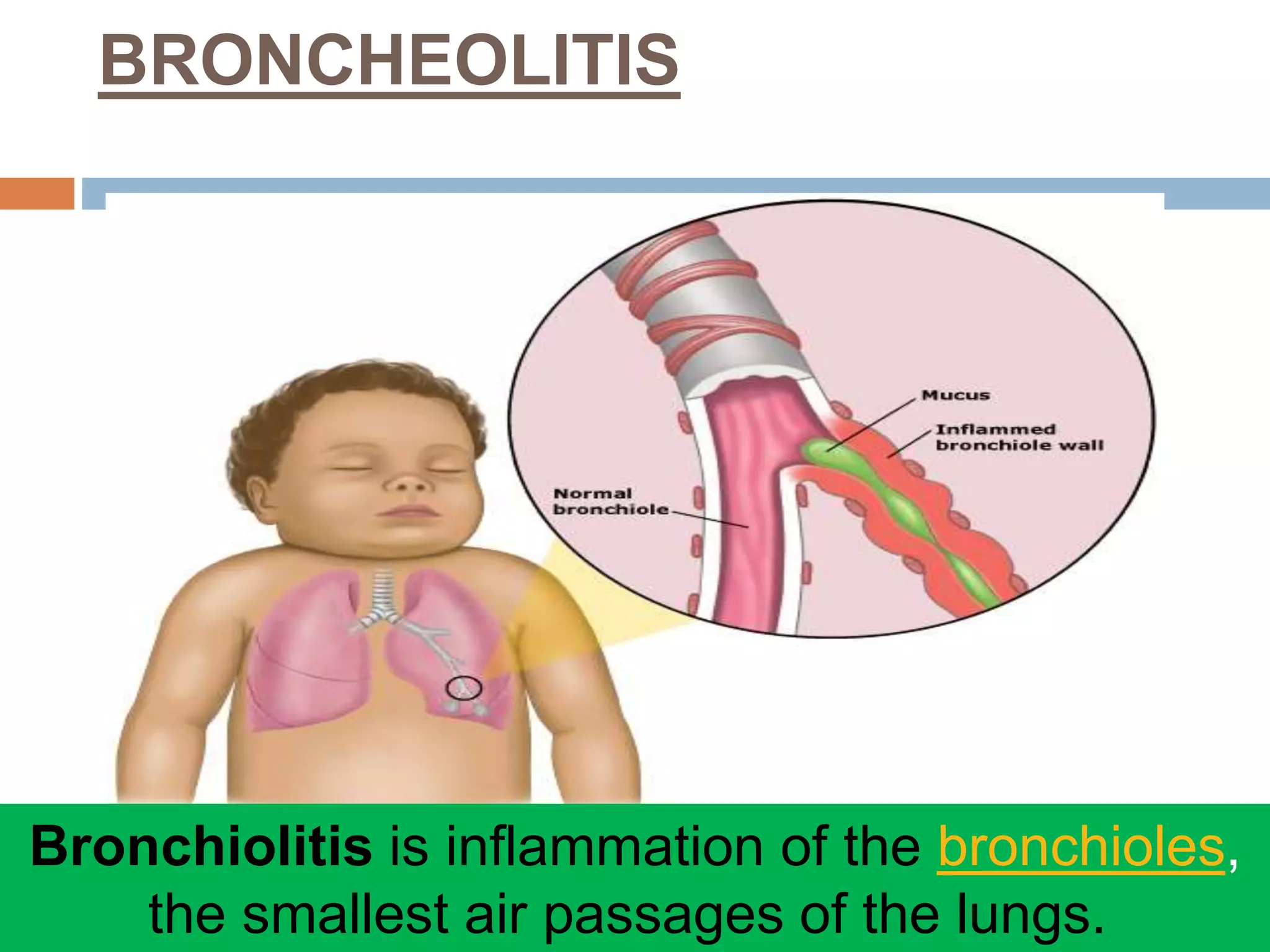






The document provides a comprehensive overview of respiratory disorders relevant to child health nursing, detailing conditions such as tonsillitis, choanal atresia, epistaxis, bronchiolitis, and bronchopneumonia. It covers the definitions, causes, pathophysiology, clinical manifestations, diagnosis, and management of these disorders. Emphasis is placed on proper nursing care, surgical interventions, and preventive measures for respiratory health in children.























































































