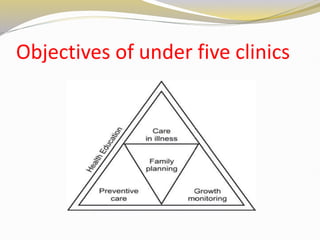
The document discusses preventive pediatrics and the role of nurses. It defines preventive pediatrics as preventing disease, promoting health, and maintaining well-being in children. The aims include preventing, detecting, and treating diseases early to avoid complications. Aspects discussed include growth monitoring, immunizations, nutrition programs, and health education. It outlines the types and levels of prevention including primary, secondary, and tertiary. The conclusion discusses the nurse's role in areas like health education, immunizations, breastfeeding promotion, and participating in child health programs.








![DEFINITION
Cold chain is a system of storage and transport of
vaccines at optimum temperature [2-8 °c] from
manufacture to the site of vaccination. This cold chain
is needed because vaccines are sensitive to heat and
they may lose their potency if not stored and
transported at optimum temperature.](https://image.slidesharecdn.com/cdfbui8bq9gkk27m95nw-c2bd3bc6-bce4-4c2a-b0f4-440a8d663caf-240415145552-41992a0f/85/Preventive-pediatrics-aspects-types-level-of-care-37-320.jpg)