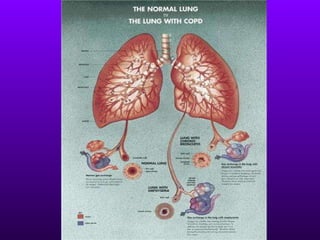
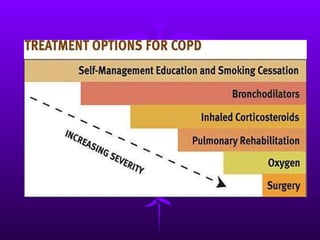
COPD is a progressive lung disease defined by abnormal airflow that worsens over time. It encompasses chronic bronchitis and emphysema and is usually caused by smoking or air pollution. Symptoms include a chronic cough, shortness of breath, wheezing and chest tightness. Diagnosis involves lung function tests showing reduced airflow. Treatment focuses on stopping smoking and medications to relieve symptoms.