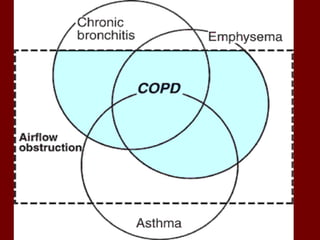
1. Chronic obstructive pulmonary disease (COPD) is a slowly progressive disorder characterized by airway obstruction including chronic bronchitis and emphysema.
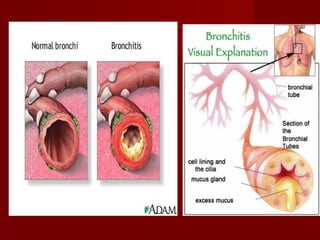
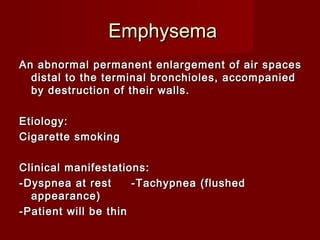
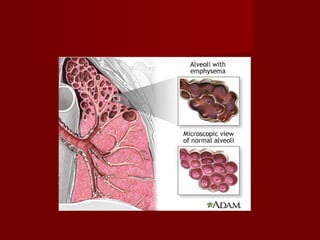
2. Chronic bronchitis involves excessive mucus production and airway obstruction for at least 3 months per year for 2 years. Emphysema involves the abnormal enlargement of air spaces in the lungs.
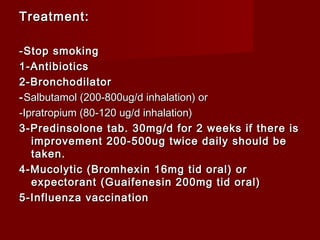
3. Cigarette smoking is a leading cause of COPD and its management involves bronchodilators, steroids, antibiotics and smoking cessation.