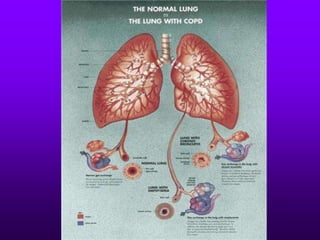
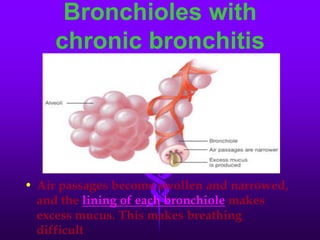
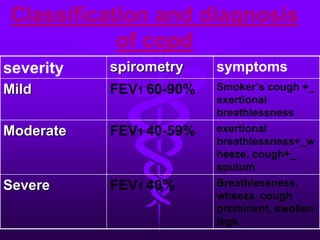
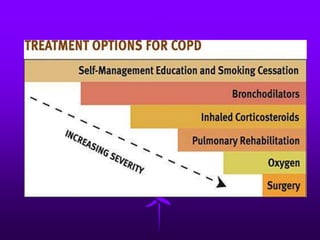
Chronic obstructive pulmonary disease (COPD) is a progressive lung disease characterized by airflow obstruction and breathlessness. It encompasses chronic bronchitis and emphysema and is usually caused by smoking. Symptoms include chronic cough, sputum production, shortness of breath, wheezing and chest tightness. Diagnosis involves lung function tests showing reduced airflow and chest imaging may show signs of emphysema like bullae. Treatment focuses on smoking cessation and medications can provide short-term relief of exacerbations and long-term management of symptoms.
































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







