Download to read offline





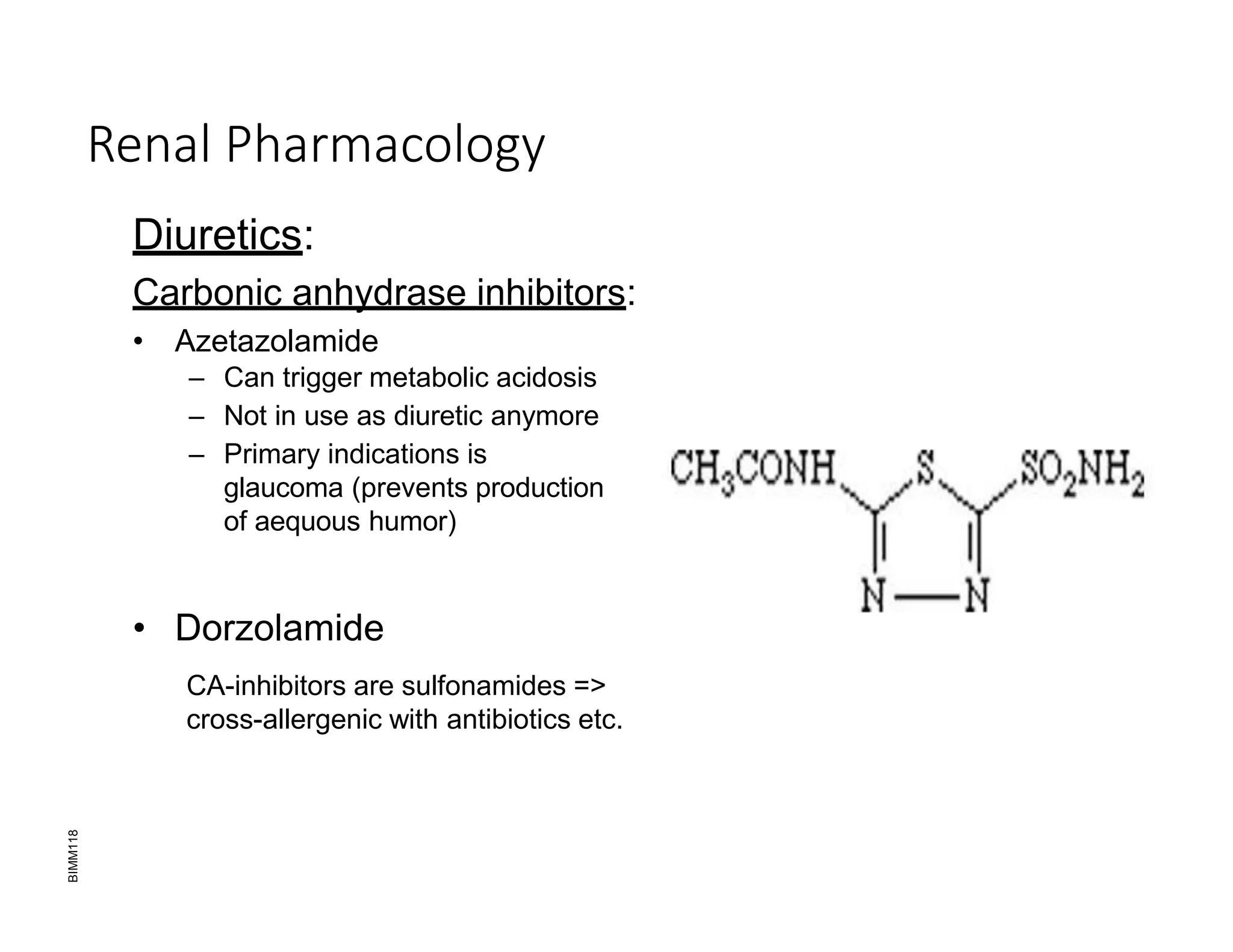

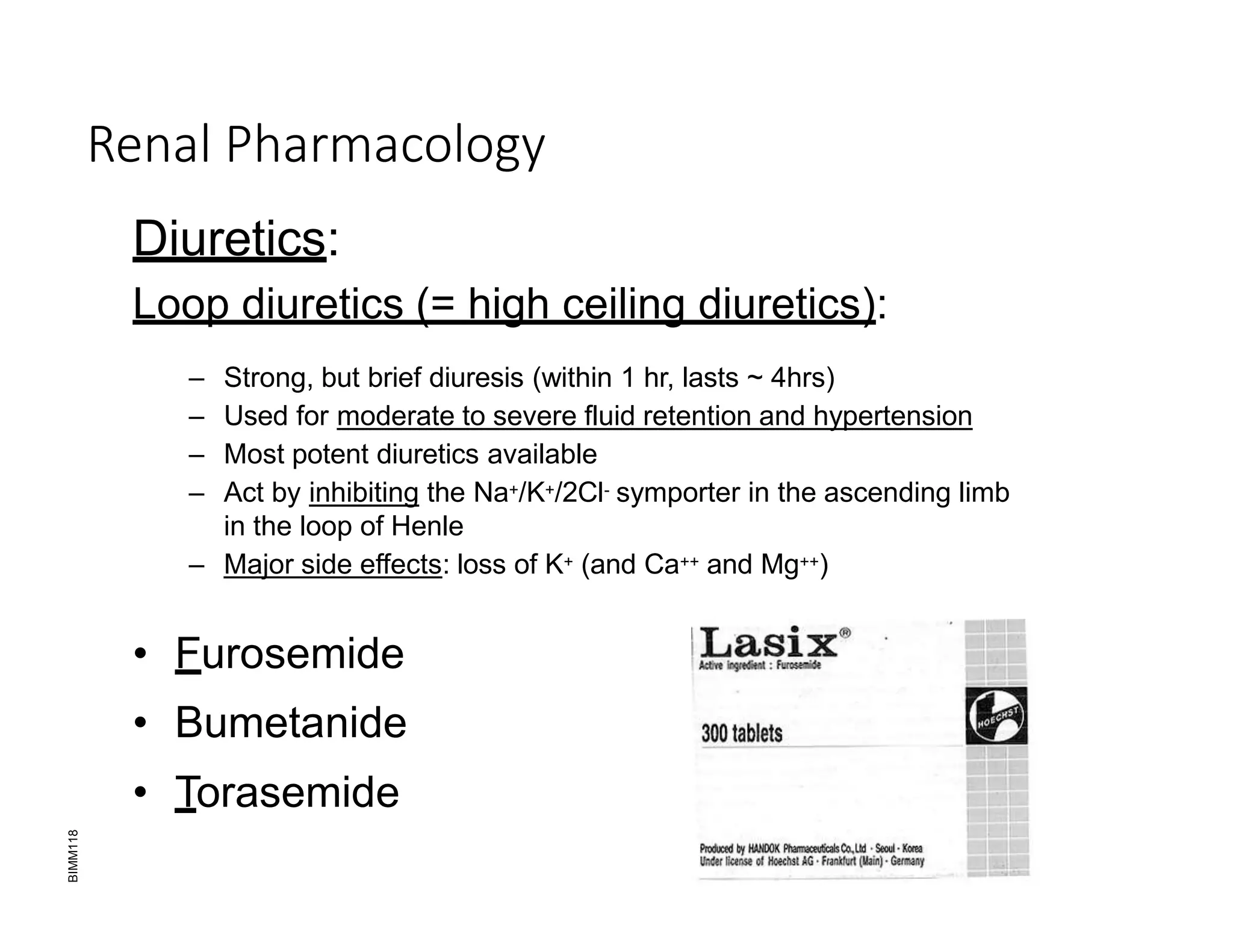


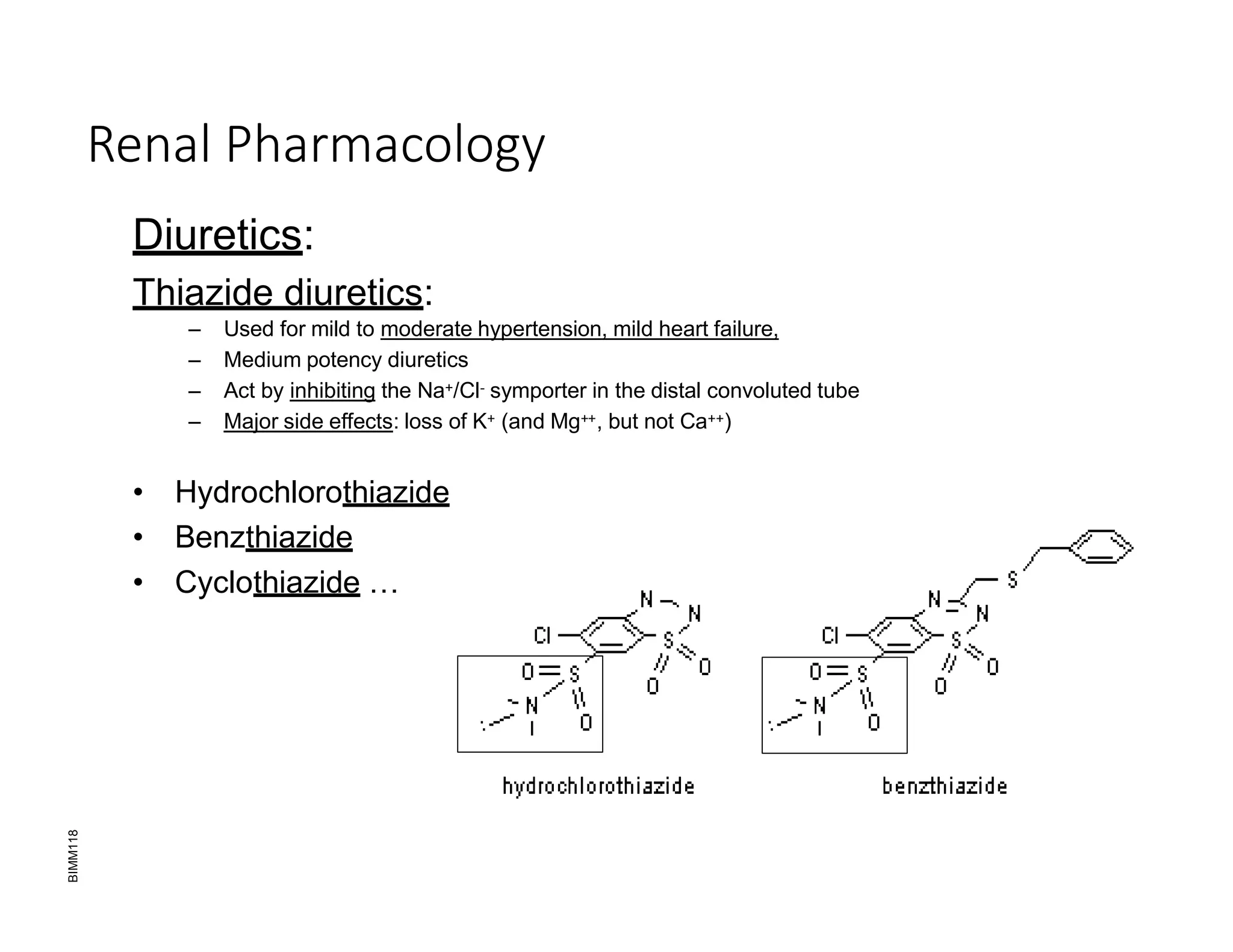




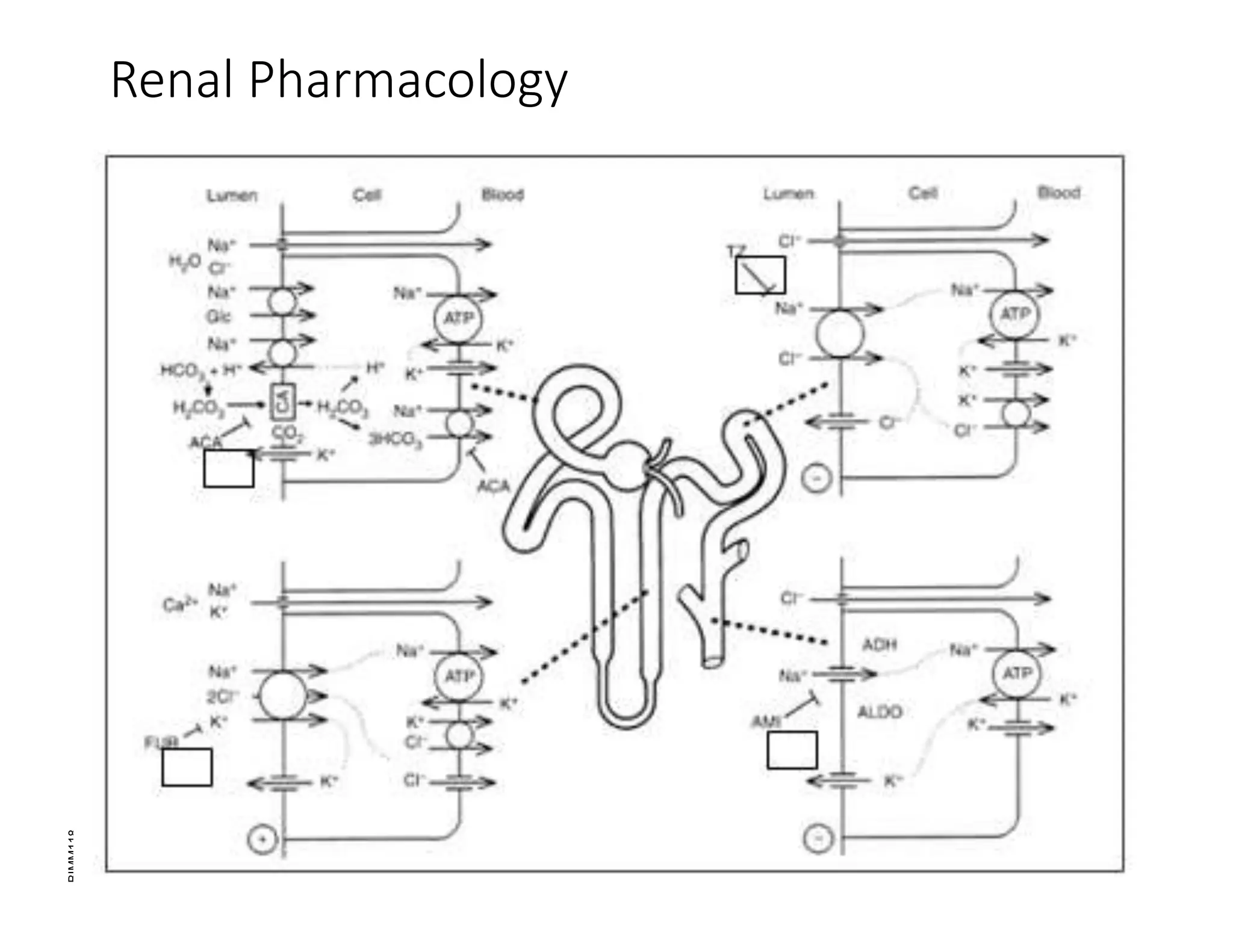


The document discusses renal pharmacology, focusing on diuretics that affect kidney function, including their mechanisms, types, and side effects. Diuretics are primarily used to manage hypertension and fluid retention by blocking sodium and chloride reabsorption, leading to increased urine output. Additionally, it outlines the roles of the kidneys in maintaining fluid balance and highlights complications associated with uric acid and its relevance to conditions like gout.























































































