Downloaded 192 times
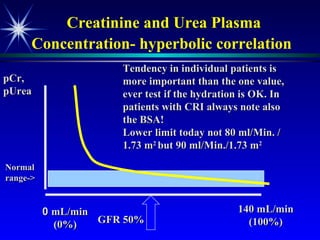
![Plasma creatinine vs. GFR not linear, hyperbolic correlation! GFR [pCreat] 140 mL/min (100%) 0 mL/min (0%) Change within an individual patient is usually more important than the absolute value](https://image.slidesharecdn.com/renalfunctionsinchildren-100330004306-phpapp02/85/Renal-Functions-In-Children-22-320.jpg)

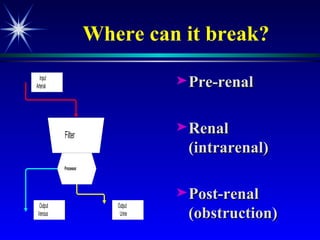
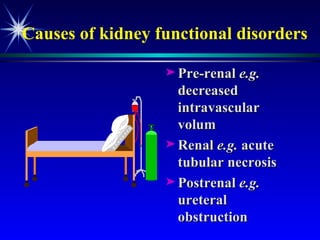
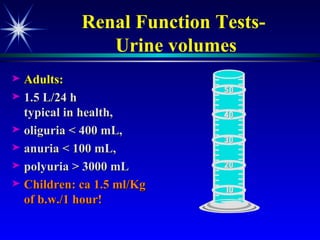
The document discusses various tests used to evaluate renal function, including tests of glomerular filtration rate (GFR) and clearance tests. It describes how the kidney regulates water, electrolytes, and acid-base balance and produces hormones. Laboratory tests discussed include measures of creatinine, urea, urine output, protein, and osmolality. Causes of impaired kidney function are categorized as pre-renal, renal, or post-renal.




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

