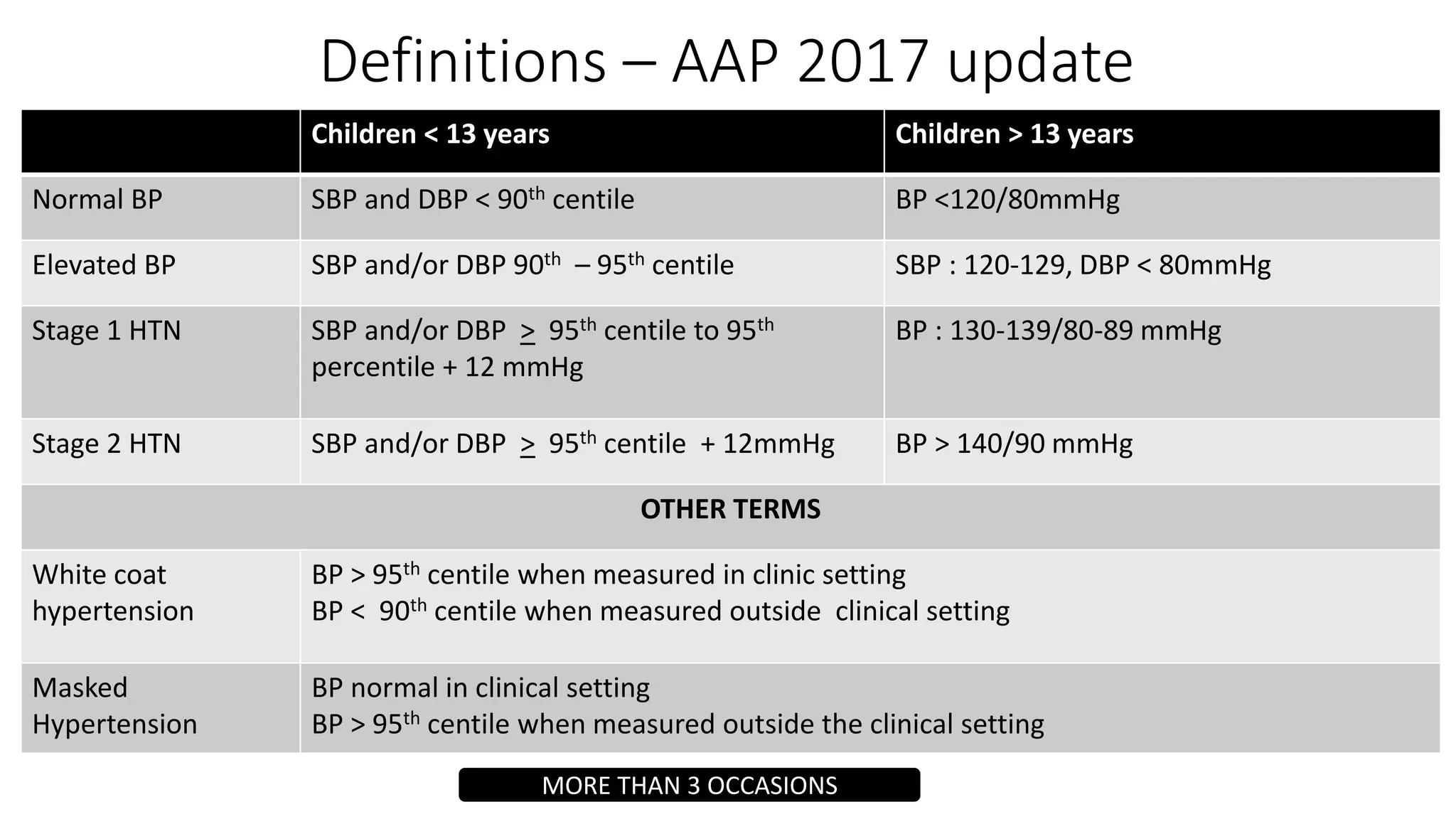
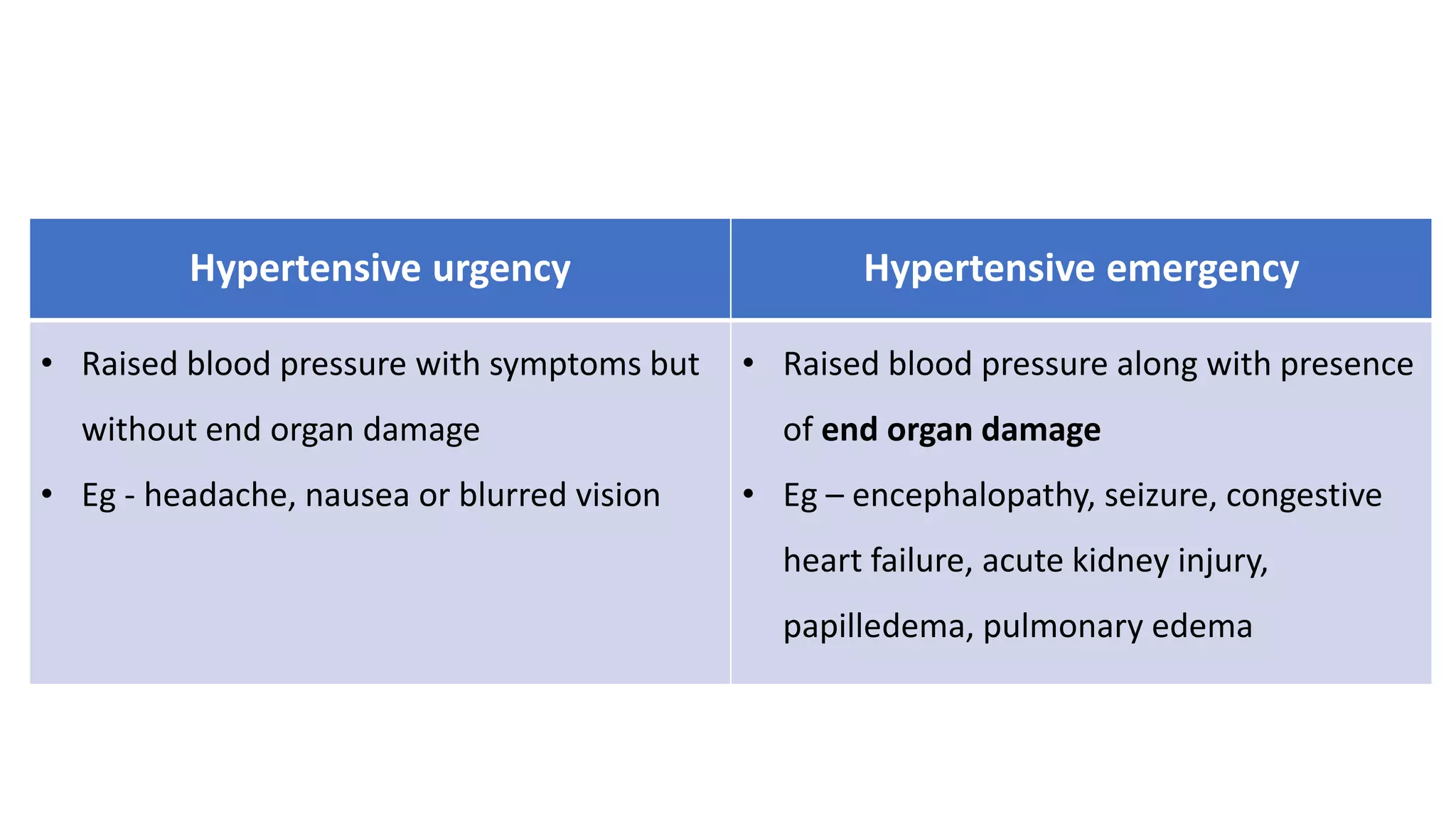
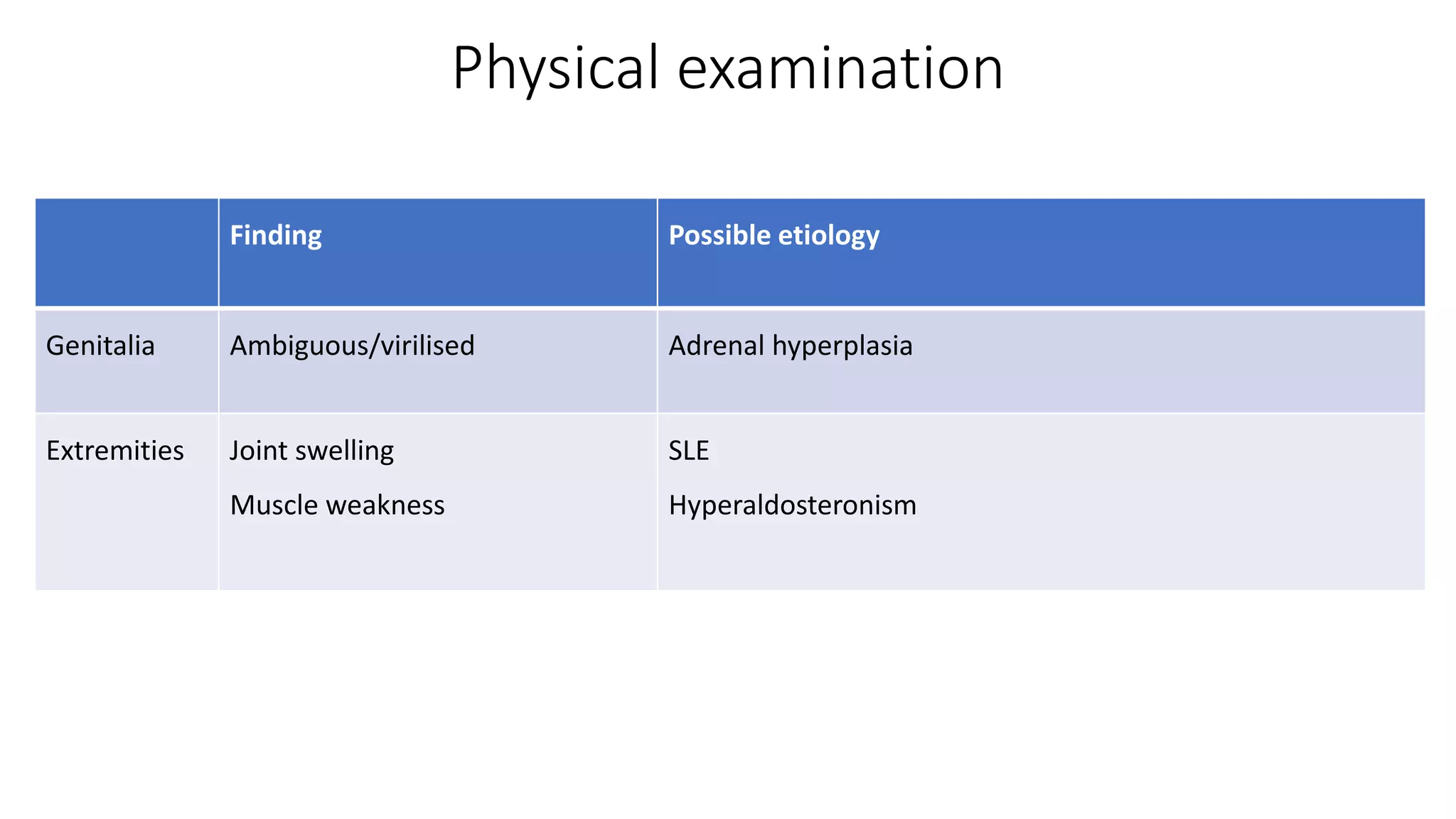
This document provides guidelines for the diagnosis and management of pediatric hypertension. It discusses definitions of hypertension in children, prevalence related to obesity, secondary causes including renal and endocrine issues, evaluation involving history, exam, and testing, and treatment focusing on lifestyle changes and medication if needed. The goal is to lower blood pressure to less than the 90th percentile to prevent end organ damage and future cardiovascular disease.