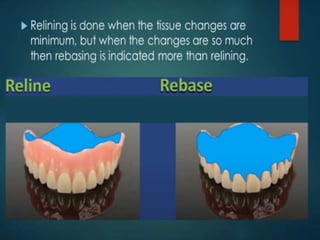
1. Dentures need to be relined periodically, usually every 2-3 years, to account for residual ridge resorption which causes dentures to become loose.
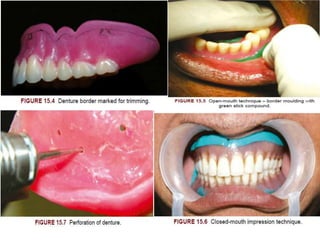
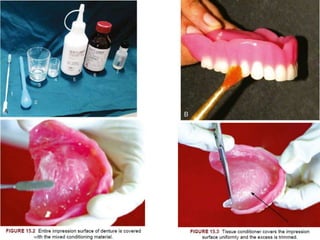
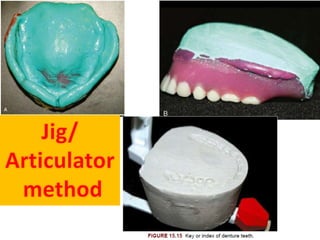
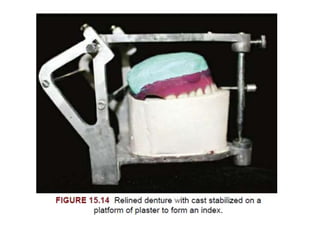
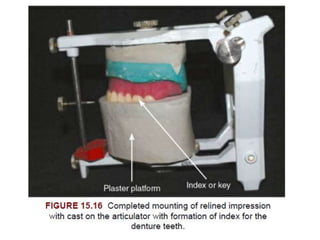
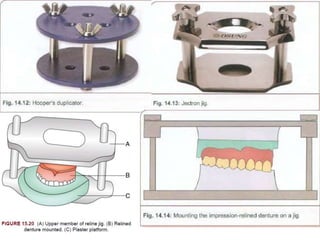
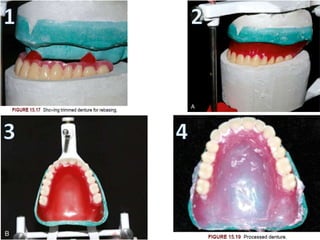
2. The relining process involves taking a new impression using the existing denture and replacing the impression material with denture base material in the lab.
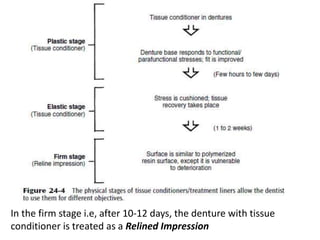
3. Common materials used for the relining impression include zinc oxide eugenol, rubberbase impressions, and tissue conditioners. The functional reline technique uses tissue conditioners.




















![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)















































