Relining and Rebasingin complete denture
Dr. Saee Deshpande Dr. N. A. Pande Dr. Rajlakshmi Banerjee
Guide and Professor HOD and Professor Reader
Dr. Anuj Chandak Dr. Akhil Rathi Dr. Priti Jaiswal
Reader Reader Reader
Presented by-
Dr. Divya Kamnani
MDS I year
25/03/2025
Introduction
•Adaptation of thedenture bases to the mucosa that covers the residual ridges is a critical part of a
complete denture service.
•Every edentulous patient should be examined on an annual basis to determine (among other
things) the rate of resorption of the residual ridges.
•There is some clinical evidence to suggest that the rate of osseous change can be retarded when
complete dentures are readapted to the residual ridges at the first signs and symptoms of loss of
adaptation.
4.
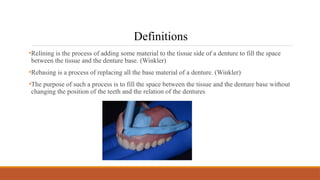
•Relining is theprocess of adding some material to the tissue side of a denture to fill the space
between the tissue and the denture base. (Winkler)
•Rebasing is a process of replacing all the base material of a denture. (Winkler)
•The purpose of such a process is to fill the space between the tissue and the denture base without
changing the position of the teeth and the relation of the dentures
Definitions
5.
• Reline- isthe procedures used to resurface the inatglio of removable dental prosthesis with new base
material, thus producing an accurate adaptationto the denture foundation area. (GPT 10)
• Rebase- is the laboratory process of replacing the entire denture base material on an existing
prosthesis. (GPT 10)
Excessive amount ofresorption
Contraindication
s
Patient complains of
temporomandibular joint
problems
Dentures create a major speech
problem.
Abused soft tissues are present
Dentures have poor esthetics or
unsatisfactory jaw relationships.
Severe osseous undercuts exist
8.
General considerations
1) Satisfactoryvertical
dimension of occlusion
2)Centric occlusion should
coincide with Centric
relation
3)Acceptable patient
apperance
4) Oral tissues in optimum
health
5) Posterior limit of
maxillary denture is correct.
9.
6)Denture base extension
areadequate.
7) Adequate load
distribution on basal seat.
8)Interocclusal distance is
correct.
9) Satisfactory speech
10) There are no existing
hard or soft tissue
conditions that would
preclude the technique.
10.
Preparatory phase
Tissue preparation
1.Excessive hypertrophic tissue should be surgically removed.
2. The oral mucosa should be free of irritation.
3. Removal of the dentures from the mouth during sleep
4. The dentures should be left out of the mouth - 2- 3 weeks before.
5. Daily massage of the soft tissues.
11.
Denture preparation
1. Pressureareas on the tissue surface of the dentures should be relieved.
2. Minor occlusal disharmony is corrected by selective grinding.
3. Small border inadequacies are corrected.
4. A correct posterior palatal seal area should be established before the final impression.
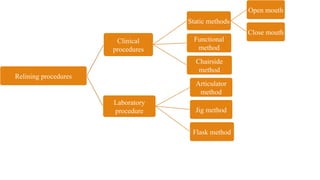
Clinical procedures- Staticmethod
•Dentures are used essentially as trays for making the new impressions.
•Relining/rebasing of both maxillary and mandibular dentures can be done at the same
appointment.
•The existing CO is not used, and a new CRO record is obtained after the impressions are made.
•Tissue surface and borders of denture are removed around 1- 2mm.
• Tissue stops are prepared in denture using low fusing compund.
Open mouth technique - (Carl
O Boucher)
14.
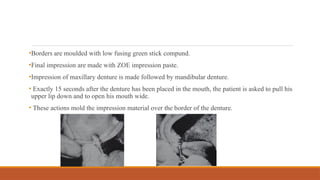
•Borders are mouldedwith low fusing green stick compund.
•Final impression are made with ZOE impression paste.
•Impression of maxillary denture is made followed by mandibular denture.
• Exactly 15 seconds after the denture has been placed in the mouth, the patient is asked to pull his
upper lip down and to open his mouth wide.
• These actions mold the impression material over the border of the denture.
15.
• Selective trimminghelps to make a
selective pressure impression.
• Making a separate inter-occlusal
record will allow the operator to
concentrate on recording the jaw
relation.
• It is possible to verify the centric
relation record if necessary.
• The inter-occlusal record is reliable.
Advantages
• Difficult procedure.
• It requires more clinical and
laboratory time
Disadvantages
16.
Closed mouth Reliningtechniques - Maxillary denture
•In the closed mouth variation, the dentures are used as impression trays and either the existing
CRO is used to seat the dentures with lining impression material or else the CR is recorded(in the
registration medium of choice) before the impressions are made.
•Various techniques have been explained.
• Technique A
• Technique B
• Technique C
• Technique D
17.
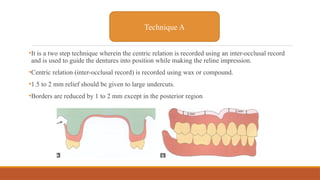
•It is atwo step technique wherein the centric relation is recorded using an inter-occlusal record
and is used to guide the dentures into position while making the reline impression.
•Centric relation (inter-occlusal record) is recorded using wax or compound.
•1.5 to 2 mm relief should be given to large undercuts.
•Borders are reduced by 1 to 2 mm except in the posterior region
Technique A
18.
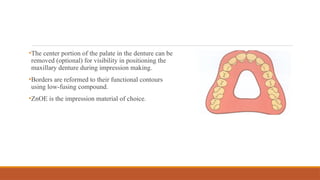
•The center portionof the palate in the denture can be
removed (optional) for visibility in positioning the
maxillary denture during impression making.
•Borders are reformed to their functional contours
using low-fusing compound.
•ZnOE is the impression material of choice.
19.
•Palatal opening willallow better seating
• Pre-made inter-occlusal record helps to
position the denture during impression
making.
• It reduces the possibility of moving the
maxillary denture forward during final
impression making.
• The wax interocclusal record is not an
accurate and safe record.
• This technique does not suggest any
solution for difficulties of relining both
dentures at the same time.
Advantages Disadvantages
20.
•No new centricrelation record is made here.
•Denture is prepared.
•Border moulding is done using low fusing compound.
•Impression wax (Iowa wax) is the material of choice for making
impressions.
•Impression is made in two stages. In the first step all areas except the
labial flange and the alveolar crest in-between the canines are recorded.
•The labial flange and alveolar crest between canines are recorded in the
second step.
Technique B
21.
• It willreduce the possibility of extreme
forward movement of the maxillary
denture.
Advantages
• Wax impression materials are difficult
to work with and can distort easily.
• If the existing centric relation record is
wrong then the impression becomes
inaccurate.
Disadvantages
22.
•Centric relation recordis obtained as in Technique B.
•The denture is prepared.
•Labial and palatal flanges are perforated to decrease the pressure inside dentures during
impression making.
Technique C
23.
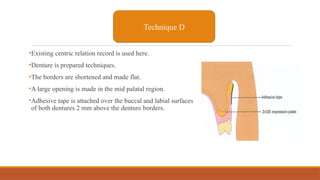
•Existing centric relationrecord is used here.
•Denture is prepared techniques.
•The borders are shortened and made flat.
•A large opening is made in the mid palatal region.
•Adhesive tape is attached over the buccal and labial surfaces
of both dentures 2 mm above the denture borders.
Technique D
24.
Dental plaster orZnOE is suggested for recording most
areas and plaster of Paris is used to record the palatal
portion.
After impression making, a deep groove is cut into labial
and buccal surfaces of the dentures at the junction of the
impression material and is filled with molten wax.
The wax at the edge of the denture is used to record the
sulcus
25.
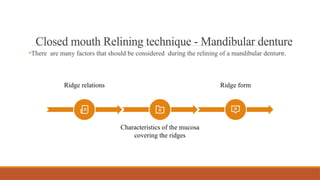
•There are manyfactors that should be considered during the relining of a mandibular denture.
Closed mouth Relining technique - Mandibular denture
Ridge relations Ridge form
Characteristics of the mucosa
covering the ridges
26.
Centric relation -The existing centric occlusion is used.
Special Suggestion:-
1) Loss of vertical dimension corrected by luting softened modeling compound to the occlusal
surfaces of the mandibular posterior teeth.
2) Patient asked to repeatedly pronounce letter “m.”
3) Record is chilled, trimmed and slightly heated before returning to the patient’s mouth.
Repeat procedure until correct occlusal vertical dimension is established to the
operator’s satisfaction.
27.
•Lower working impressionmade and poured and lower denture mounted on an articulator.
5) Denture removed and cleaned and excessive undercuts removed and is luted to the maxillary
denture in maximum intercuspation.
6) Softened modeling compound is placed inside the mandibular denture and the articulator
closed against the lower cast to contact the incisal guide pin.
7) With this procedure, the amount of vertical dimension indicated by the thickness of the
compound on the surface of the mandibular teeth is transferred to the base of the mandibular
denture.
8) Mandibular denture now is used as a tray for making the final impression.
•Impression- Modeling compound at the early stage and zinc oxide-eugenol for making the
secondary impression are suggested.
28.
• The lossof vertical dimension can
be compensated for during relining
procedures.
• The error in centric occlusion can be
reduced during the laboratory
stages.
ADVANATAGES
• Time consuming
• The procedure for establishment of
occlusal vertical dimension is
questionable.
DISADVANTAGES
29.
Functional method
• Herethe patient need not be without dentures unlike previous techniques (i.e. dentures are not
required for laboratory procedures)
•Fluid resins (tissue conditioners) are used as impression material.
•Tissue conditioners are temporary soft liners with the following characteristics:
• Easy to use.
• Excellent for refitting complete dentures.
• Capable of retaining for many weeks.
• Good in dimensional stability.
• Good in bonding to resin denture bases.
30.
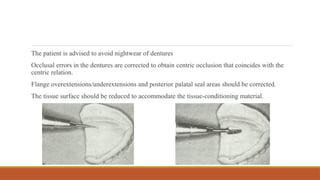
The patient isadvised to avoid nightwear of dentures
Occlusal errors in the dentures are corrected to obtain centric occlusion that coincides with the
centric relation.
Flange overextensions/underextensions and posterior palatal seal areas should be corrected.
The tissue surface should be reduced to accommodate the tissue-conditioning material.
31.
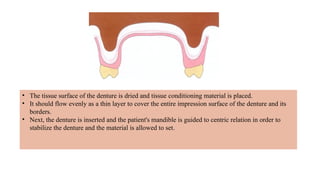
• The tissuesurface of the denture is dried and tissue conditioning material is placed.
• It should flow evenly as a thin layer to cover the entire impression surface of the denture and its
borders.
• Next, the denture is inserted and the patient's mandible is guided to centric relation in order to
stabilize the denture and the material is allowed to set.
32.
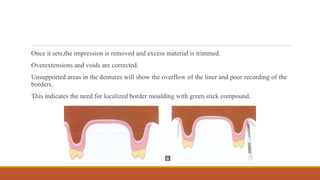
Once it sets,theimpression is removed and excess material is trimmed.
Overextensions and voids are corrected.
Unsupported areas in the dentures will show the overflow of the liner and poor recording of the
borders.
This indicates the need for localized border moulding with green stick compound.
33.
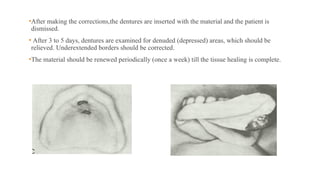
•After making thecorrections,the dentures are inserted with the material and the patient is
dismissed.
• After 3 to 5 days, dentures are examined for denuded (depressed) areas, which should be
relieved. Underextended borders should be corrected.
•The material should be renewed periodically (once a week) till the tissue healing is complete.
34.
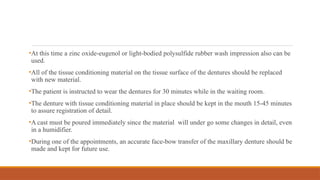
•At this timea zinc oxide-eugenol or light-bodied polysulfide rubber wash impression also can be
used.
•All of the tissue conditioning material on the tissue surface of the dentures should be replaced
with new material.
•The patient is instructed to wear the dentures for 30 minutes while in the waiting room.
•The denture with tissue conditioning material in place should be kept in the mouth 15-45 minutes
to assure registration of detail.
•A cast must be poured immediately since the material will under go some changes in detail, even
in a humidifier.
•During one of the appointments, an accurate face-bow transfer of the maxillary denture should be
made and kept for future use.
35.
Chair- side technique
•Thismethod makes use of acrylic that could be added to the denture and allowed to set in the
mouth for relining/rebasing.
•Disadvantages-
1. The materials often produce a chemical burn on the mucosa.
2. The result is porous and develops a bad odour.
3. Material is not easy to remove .
4. Poor colour stability.
36.
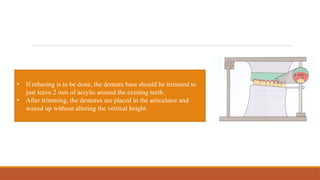
• If rebasingis to be done, the denture base should be trimmed to
just leave 2 mm of acrylic around the existing teeth.
• After trimming, the dentures are placed in the articulator and
waxed up without altering the vertical height.
37.
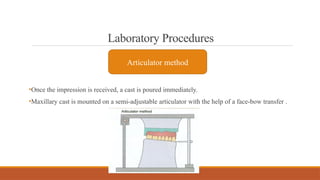
Laboratory Procedures
•Once theimpression is received, a cast is poured immediately.
•Maxillary cast is mounted on a semi-adjustable articulator with the help of a face-bow transfer .
Articulator method
38.
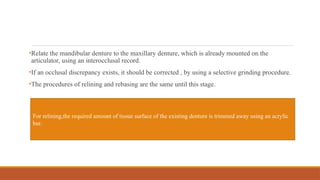
•Relate the mandibulardenture to the maxillary denture, which is already mounted on the
articulator, using an interocclusal record.
•If an occlusal discrepancy exists, it should be corrected , by using a selective grinding procedure.
•The procedures of relining and rebasing are the same until this stage.
For relining,the required amount of tissue surface of the existing denture is trimmed away using an acrylic
bur.
39.
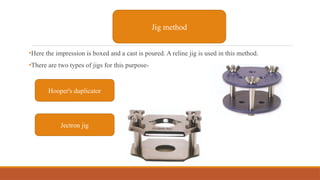
•Here the impressionis boxed and a cast is poured. A reline jig is used in this method.
•There are two types of jigs for this purpose-
Jig method
Hooper's duplicator
Jectron jig
40.
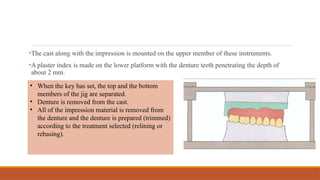
•The cast alongwith the impression is mounted on the upper member of these instruments.
•A plaster index is made on the lower platform with the denture teeth penetrating the depth of
about 2 mm.
• When the key has set, the top and the bottom
members of the jig are separated.
• Denture is removed from the cast.
• All of the impression material is removed from
the denture and the denture is prepared (trimmed)
according to the treatment selected (relining or
rebasing).
41.
•The trimmed denturesare then set into the plaster key and the top of the instrument is replaced.
•The denture is waxed to the cast, processed and finished as usual.
•The denture is cured in a pressure container of warm water at 15 psi for 30 minutes.
•The cured denture should be repositioned on the jig to correct the occlusion prior to insertion.
42.
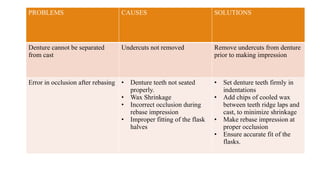
PROBLEMS CAUSES SOLUTIONS
Denturecannot be separated
from cast
Undercuts not removed Remove undercuts from denture
prior to making impression
Error in occlusion after rebasing • Denture teeth not seated
properly.
• Wax Shrinkage
• Incorrect occlusion during
rebase impression
• Improper fitting of the flask
halves
• Set denture teeth firmly in
indentations
• Add chips of cooled wax
between teeth ridge laps and
cast, to minimize shrinkage
• Make rebase impression at
proper occlusion
• Ensure accurate fit of the
flasks.
43.
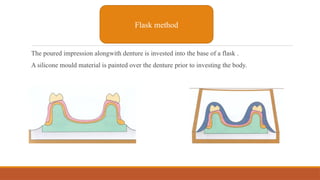
The poured impressionalongwith denture is invested into the base of a flask .
A silicone mould material is painted over the denture prior to investing the body.
Flask method
44.
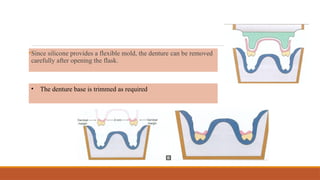
•Since silicone providesa flexible mold, the denture can be removed
carefully after opening the flask.
• The denture base is trimmed as required
45.
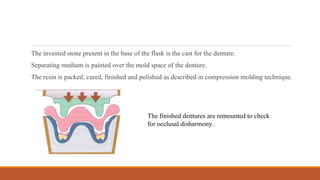
The invested stonepresent in the base of the flask is the cast for the denture.
Separating medium is painted over the mold space of the denture.
The resin is packed, cured, finished and polished as described in compression molding technique.
The finished dentures are remounted to check
for occlusal disharmony.
46.
Problem areas
• Noduleson tissue surface of dentures.
• Incorrect occlusion.
Causes
• Air incorporated in silicone during mixing.38
• Flasks do not fit properly
• Resin not packed adequately.
• Initial impression not related to proper jaw relation.
47.
Solution
• Do notwhip air into mix during mixing resin.
• Use accurately fitting flasks.
• Eliminate all flash by trial closures.
• Make sure that impression is related to proper occlusal position.
• Examine impression for damage that may occur during transit.
48.
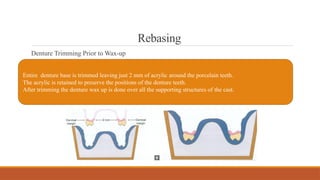
Rebasing
Denture Trimming Priorto Wax-up
Entire denture base is trimmed leaving just 2 mm of acrylic around the porcelain teeth.
The acrylic is retained to preserve the positions of the denture teeth.
After trimming the denture wax up is done over all the supporting structures of the cast.
49.
Indications
When tissue damageis
excessive
If the vertical
dimension of the
patient is changed
Can be done
properly only in
dentures with
porcelain teeth.
Hard reline materials
•Thesematerials are commomly used to provide a ‘chairside’ reline to the denture.
•Cold cure resin comes in two types.
•Major difference is in liquid content.
•Type 1 contains METHYMETHACRYLATE MONOMER while type 2 contains
BUTYLMETHACRYLATE MONOMER.
MATERIALS USED-
1. Cold cure acrylic resin
2. Heat- cured acrylic
53.
• Reasonable estheticquality.
• One appointment procedure.
• Easy to process.
• Low density.
• Good bonding with old denture.
• Saves lab cost.
Advantages
• Susceptible to distortion.
• Low thermal conductivity.
• Methylmethacrylate monomer can be
irritant to soft tissues and can sensitize
the patient.
• Have low Tg ( glass transition
temperature) which leads to increased
dimensional instability.
Disadvantages
54.
Tissue conditioners
•When softtissues have become traumatized due to wearing an ill-fitting denture, it is better to let
the tissues recover before recordind impressions for few new dentures.
•Ideally the patient should be refrained from wearing the denture but this is generally not accepted
by the patient.
• So tissue conditioners can employed to overcome the problem.
55.
Presentations are communicationtools that can be used as
demonstrations.
Your title here
Presentations are communication tools that can be used as
demonstrations.
Your title here
Composition
LIQUID
POWDER
Polymethylmethacrylate
Ethyl alcohol ( solvent)
Butylphthalate
Butylglycolate ( Plasticizer)
56.
Requirements-
• It shouldbe resilient.
• It should remain soft.
• It should flow under constant force.
• It should have high tack.
• Can be used in chair side technique.
• Improves denture fit.
• Non irritant.
ADVANTAGES
• Low cohesive strength.
DISADVANTAGES
57.
Soft lining materials
•Theseare resilient polymers used to replace the fitting surface of a hard plastic denture because
either-
1. The patient cannot tolerate hard fitiing denture.
2. To improve retention of denture.
•Soft lining materials can be divided as
1. Temporary
2. Permanent
Advantages
1) Bonds wellto acrylic.
2)Resonable resistance to damage by
denture cleansers.
3) High rupture strenght.
Disadvantages
1)Poor resiliency.
2)Loses plasticizer with time.
60.
Uses
•Can be usedin place of tissue conditioner.
•They can be used temporarily improving the fit of an ill- fitting denture until a new denture can
be constructed.
• The plasticizer gradually leasches out and liner becomes stiff as it looses its resilience.
• This depends to some extent on patients regime for cleaning denture.
• In general high temperature and strong bleaching agents should be avoided.
HEAT CURE ACRYLICMATERIAL (POLYMERIZABLE PLASTICICER
SYSTEMS)
• The material is hard at room temperature, which makes it easy to finish and softens when taken up to
mouth temperature (37o
C).
• They are supplied as powder and liquid.
63.
HEAT CURE SILICONES
•These products are supplied as single paste.
• COMPOSITION- 1)Polydimethysiloxane
2)Fillers
3)Initiator
ADVANTAGES
• High resiliency.
• More resistant in oral enviornment.
DISADVANTAGES
• Low tear strength
• Poor abrasion resistance.
• Leach out plasticizer over time.
64.
COLD CURE SILICONES
•Supplied as paste and liquid
• PASTE- 1)Polydimethy siloxane
2)Inert filler
• LIQUID- 1)Tetraethy silicate
2)Dibutyl tin dilaurate
65.
Ramin Mosharraf, MajidAbolhasani and Pirooz Givehchian,
Journal of Prosthetic Dentistry 2014
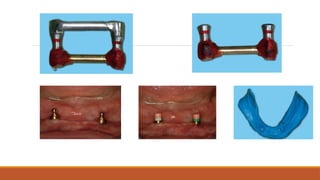
AIM- a technique for relining a mandibular bareretained overdenture that allows recording the
soft tissue beneath the bar.
67.
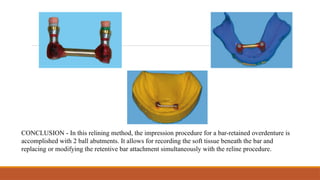
CONCLUSION - Inthis relining method, the impression procedure for a bar-retained overdenture is
accomplished with 2 ball abutments. It allows for recording the soft tissue beneath the bar and
replacing or modifying the retentive bar attachment simultaneously with the reline procedure.
68.
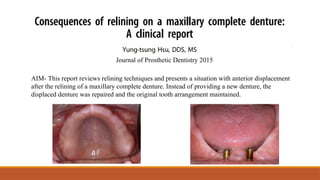
AIM- This reportreviews relining techniques and presents a situation with anterior displacement
after the relining of a maxillary complete denture. Instead of providing a new denture, the
displaced denture was repaired and the original tooth arrangement maintained.
Journal of Prosthetic Dentistry 2015
70.
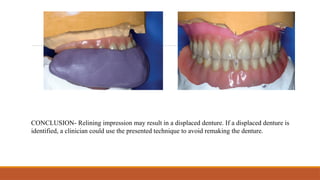
CONCLUSION- Relining impressionmay result in a displaced denture. If a displaced denture is
identified, a clinician could use the presented technique to avoid remaking the denture.
71.
AIM- This studyaimed to compare different treatment modalities to correct ill-fitted maxillary
complete denture either by the conventional relining method or by scanning the relining
impression and digitally construct a new denture regarding patient satisfaction, denture retention,
and adaptation.
BMC Oral health 2025
73.
Conclusion
•Ill-fitted maxillary completedentures corrected by conventional relining procedure showed better
esthetics, retention, and adaptation than digitally constructed maxillary dentures which showed
acceptable esthetics, retention, and adaptation with better time and data saving.
74.
Conclusion
•In conclusion, bothrelining and rebasing are vital procedures in prosthodontics aimed at
improving the fit, function, and comfort of removable dental prostheses.
•Both techniques help in maintaining the long-term effectiveness and comfort of dentures,
addressing issues such as poor fit, discomfort, and functional limitations.
•By understanding the differences and applications of these procedures, dental professionals can
provide more effective and personalized care to their patients, enhancing the overall success and
satisfaction with prosthetic rehabilitation.
75.
Questions
1)What is theprimary purpose of relining a denture?
a) To change the shape of the denture
b) To improve the fit of the denture
c) To alter the appearance of the denture
d) To repair cracks in the denture
2) When is rebasing typically performed on a denture?
a) When there is a need to replace the denture teeth only
b) When the denture base material is damaged or worn out
c) When the patient complains about the appearance of the denture
d) When there is a change in the patient's bite
76.
3) Which closemouth relining methods records the impression in two stages
a) Technique A
b) Technique B
c) Technique C
d) Technique D
4)Which of the following materials is typically used for soft relining in dentures?
a) Polyurethane
b) Acrylic resin
c) Silicone-based materials
d) Glass ionomer
77.
5) All ofthe following are indications for relining except
a) Immediate denture
b) Resorbed alveolar ridges
c) Patients who cannot afford new denture construction
d) Dentures with unsatisfactory jaw relationship.
78.
References
Winkler S. Essentialof Complete Denture Prosthodontics, 355.
Kamal MN. Comparison between relining of ill-fitted maxillary complete denture versus
CAD/CAM milling of new one regarding patient satisfaction, denture retention and adaptation.
BMC Oral Health. 2025 Jan 4;25(1):18.
Hsu YT. Consequences of relining on a maxillary complete denture: A clinical report. The
Journal of Prosthetic Dentistry. 2015 Jul 1;114(1):13-6
Mosharraf R, Abolhasani M, Givehchian P. A technique for relining bar-retained overdentures.
The Journal of Prosthetic Dentistry. 2014 Dec 1;112(6):1591-4.
Nallaswamy D. Textbook of prosthodontics. JP Medical Ltd; 2017 Sep 30.
Editor's Notes
#3 The residual ridges have been described as plastic in nature, always changing in topography and morphology from many causes, some known and many unknown.
Resorption frequently results from systemic disease.
In an ideal situation, the systemic
condition should be eliminated or controlled
before relining, rebasing, or constructing a new
denture.
#6 . Immediate dentures at three to six months after their original construction.
2. When the residual alveolar ridges have resorbed and the adaptation of the denture bases to the ridges is poor.
3. When the patient cannot afford the cost of having new dentures constructed.
4. When the construction of new dentures with the accompanying series of appointments can cause physical or mental stress, such as for geriatric or chronically ill patients.
#7 When an has taken place excessive amount of resorption.
2. When abused soft tissues are present. Then relining is not indicated until the tissues recover and return as closely as possible to normal form.
3. When the patient complains of temporomandibular joint problems. Until accurate diagnosis and treatment of the problem has been accomplished, relining or rebasing is contraindicated.
4. If the dentures have poor esthetics or unsatisfactory jaw relationships.
5. If the dentures create a major speech problem.
6. Ehen severe osseous undercuts exist, until surgical removal and healing occurs.
#9 uch as redundant tissue or severe osseous
undercuts.
#10 The dentures can be used as
a surgical splint.
#11 Stick compound and autopolymerizing acrylic resin can be used for this purpose.
#13 to maintain vertical dimension occlusal plain and aesthetic position of anterior teeth
#18 Dur_x0002_ing impression making,patient is asked to close lightly into
the newly-made inter-occlusal record. If the palatal portion
has been cut,quick setting plaster should be used to make
impression.
#19 of the denture and alleviate the increase in vertical dimension.
that the patient can close on several times without the possibility of damaging the record.
#32 The lining material will slump during setting if
not adequately supported by the denture.
#35 if not placed correctly.
if not placed correctly.
.
#38 For relining,the required amount of tissue sur_x0002_face of the existing denture is trimmed away using an acrylic
bur
#40 When the key has set, the top and the bottom members
of the jig are separated. Denture is removed from the
cast.
• All of the impression material is removed from the
dentureand thedentureisprepared (trimmed) according
to the treatment selected (relining or rebasing).
#52 mma irritant to soft tissue and can sensitize the patient.m
#55 Liquid do not conatin monomer and powder no initiater.
#56 resilient so that masticatory load are absorbed without causing permanent deformation of the lining.
Cohesive Cohesive strength is a measure of how well a material can resist being pulled apart by internal forces