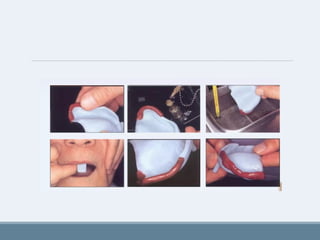
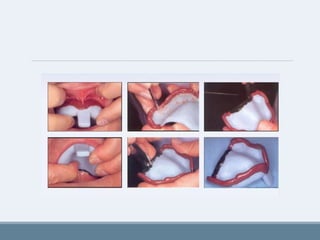
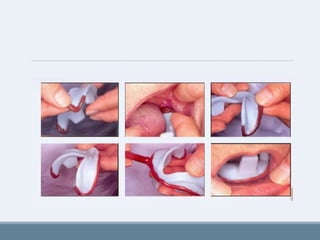
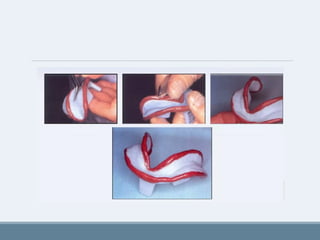
The document presents a comprehensive overview of impression techniques in complete denture fabrication, detailing fundamental rules, objectives, and classifications of various techniques such as pressure theory and minimal pressure theory. It emphasizes the importance of understanding oral anatomy, patient management, and material selection in achieving successful impressions. Additionally, it discusses the factors affecting retention, stability, and esthetics of complete dentures, alongside the steps involved in making preliminary and final impressions.