Downloaded 33 times

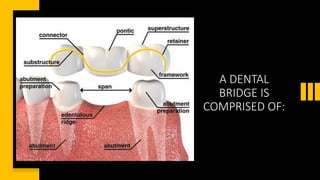

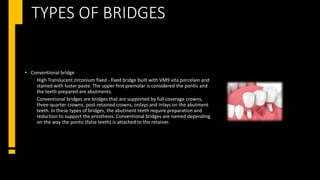



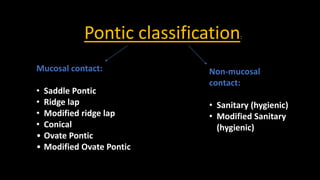
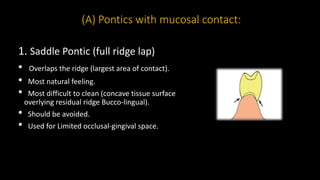
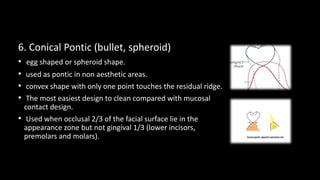
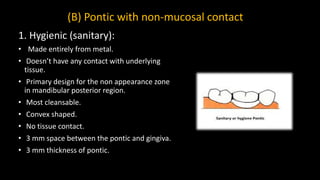
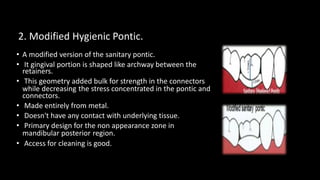
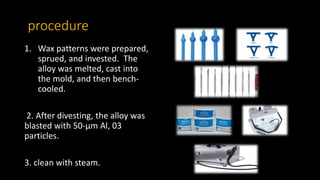

The document discusses various aspects of bridge and pontic design in dentistry, focusing on definitions, types, and materials used in fabricating dental prostheses. It describes the importance of pontics in replacing missing teeth, their design considerations, and the mechanical and aesthetic functions they serve. Additionally, it outlines different pontic designs, their classifications, and the procedures for fabrication.
![[Crown & Bridges] [terminology & classification]](https://cdn.slidesharecdn.com/ss_thumbnails/lec01-02terminologyclassification-151105130852-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)



































![/'.,mklppontics final year.pptx m,l;;[']\](https://cdn.slidesharecdn.com/ss_thumbnails/ponticsfinalyear-251031103915-60ae6a8b-thumbnail.jpg?width=640&height=640&fit=bounds)




























![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

