Downloaded 27 times
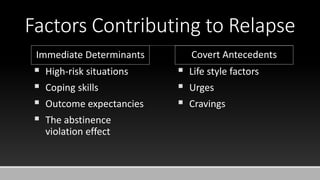
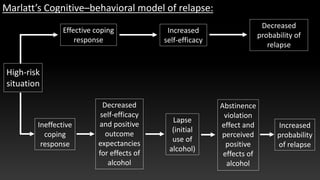
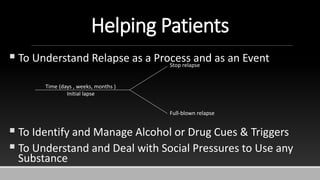

The document provides an overview of cognitive behavioral therapy (CBT) as a method for managing emotional and behavioral issues, emphasizing its role in relapse prevention (RP) for individuals recovering from substance abuse. It discusses the importance of identifying high-risk situations, developing effective coping strategies, and the cognitive-behavioral model in addressing relapses. Additionally, it highlights intervention strategies and the significance of supportive social networks in maintaining recovery.


























![Depression [2002]](https://cdn.slidesharecdn.com/ss_thumbnails/depression-170814010933-thumbnail.jpg?width=640&height=640&fit=bounds)














![Hart karern_e[1]._relapse_prevention_for_alcoholism](https://cdn.slidesharecdn.com/ss_thumbnails/hartkarerne1-170713161514-thumbnail.jpg?width=640&height=640&fit=bounds)


![Hart karern_e[1]._relapse_prevention_for_alcoholism](https://cdn.slidesharecdn.com/ss_thumbnails/hartkarerne1-relapsepreventionforalcoholism-100916174017-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Hart karern_e[1]._relapse_prevention_for_alcoholism](https://cdn.slidesharecdn.com/ss_thumbnails/hartkarerne1-relapsepreventionforalcoholism-101217225151-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



























