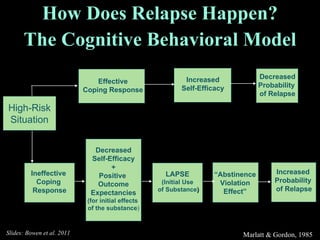






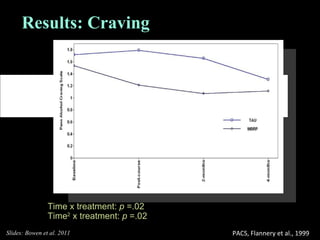
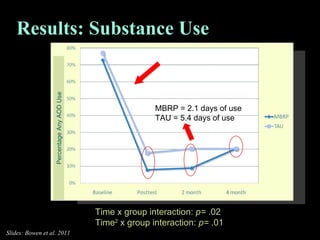



The document outlines the cognitive behavioral model of relapse and the effectiveness of relapse prevention therapy (RPT), including mindfulness-based relapse prevention (MBRP) as a treatment method. Research indicates that while RPT does not stop lapses more effectively than other treatments, it is better at delaying them and maintaining long-term treatment effects. MBRP integrates mindfulness practices to enhance awareness and acceptance, resulting in reduced craving and substance use among individuals with co-occurring disorders.































![Mindfulness and Happiness presentation [13 Jan 2016]](https://cdn.slidesharecdn.com/ss_thumbnails/thismindfulnessandhappinessv1-160115233504-thumbnail.jpg?width=640&height=640&fit=bounds)







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


