
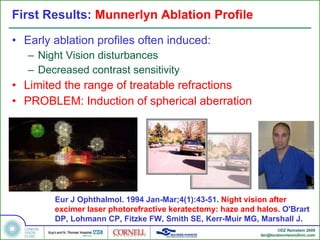
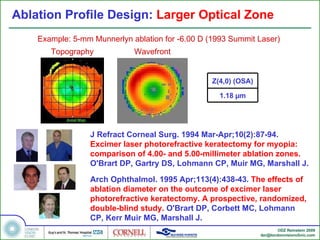
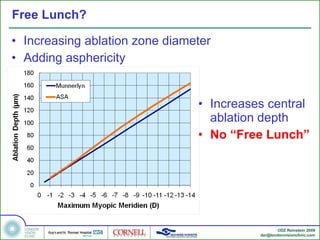
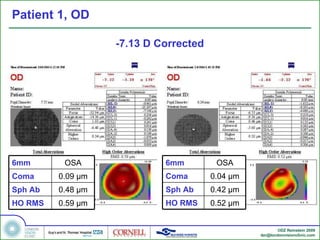
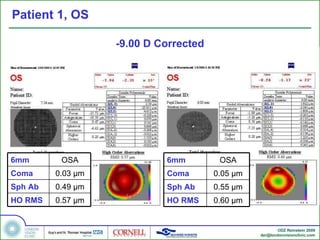
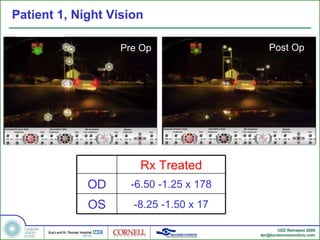
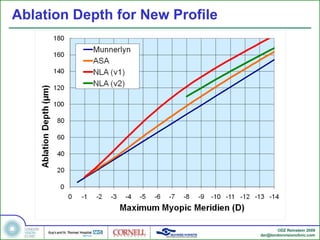
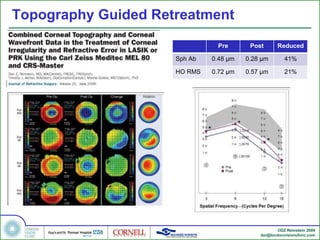
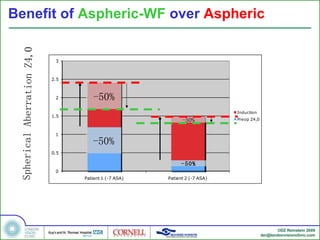

1) Early LASIK ablation profiles for high myopia induced spherical aberration and night vision disturbances. 2) Newer aspheric and wavefront-guided profiles aim to reduce spherical aberration induction but may still cause issues for high corrections. 3) A two-stage procedure using wavefront-guided or topography-guided enhancement can improve outcomes for high myopia LASIK.
























































































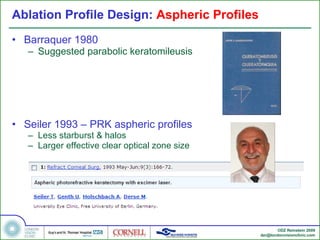
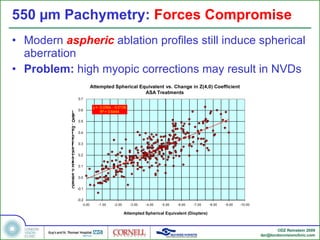
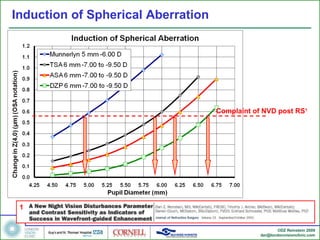
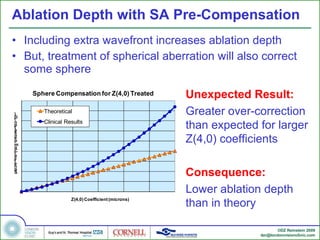
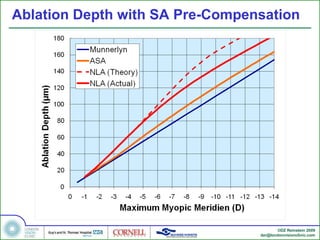
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
