Download to read offline


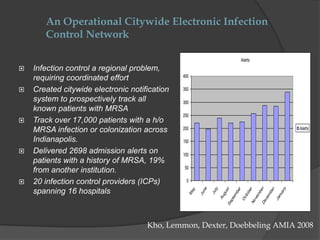




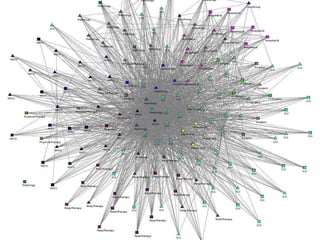



This document summarizes programs and strategies to reduce Methicillin-resistant Staphylococcus aureus (MRSA) infections. It discusses the creation of an electronic infection control network across Indianapolis hospitals to track over 17,000 patients with a history of MRSA. Through collaborative initiatives involving multiple hospitals, MRSA rates were reduced by 60-85%. The strategies discussed include fostering organizational change, engaging frontline staff, implementing standardized processes, and using data to document impact and disseminate effective practices nationally. The presentation emphasizes that change initiatives require both top-down support and bottom-up engagement from staff.



























































![Microsystem analysis webinar_feb_21_2013[1]](https://cdn.slidesharecdn.com/ss_thumbnails/microsystemanalysiswebinarfeb2120131-130220151815-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


















