Downloaded 25 times
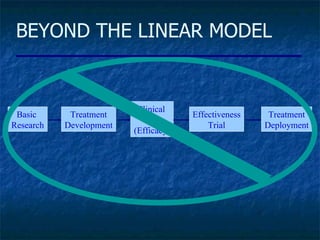



The document discusses problems with current approaches to quality improvement (QI) research and implementation science. It argues that QI research often lacks consideration of context and implementation processes. Multilevel and mixed methods designs are proposed to better account for these factors. Complexity science principles are also discussed as relevant to understanding implementation within organizational systems. The document calls for building more capacity for implementation research through multidisciplinary teams, long-term studies, and involvement of end users.