
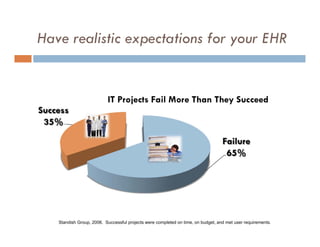
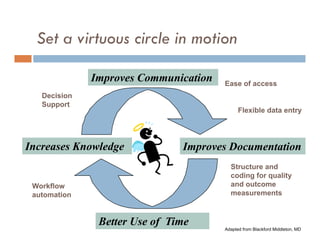
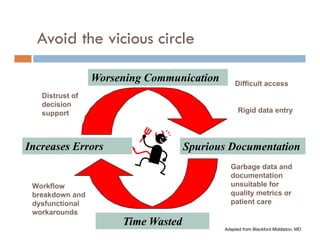
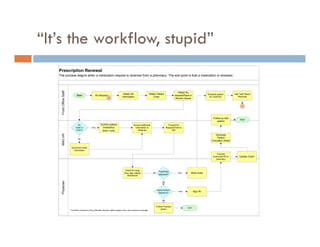
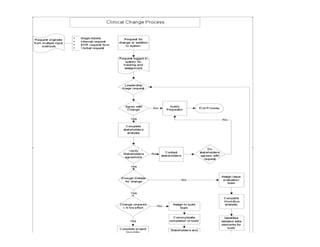


This document summarizes strategies for clinician adoption after an EHR go-live presented by Dr. Justin Graham. It recommends embedding HIT into organizational strategy, evolving governance from projects to operations, having realistic EHR expectations, setting virtuous workflow cycles, preparing for requests, learning informatics team management, and keeping vision and momentum. Culture change takes time and an engaged clinical leader, informatics team, and communication plan are important for adoption.


























































