Downloaded 17 times
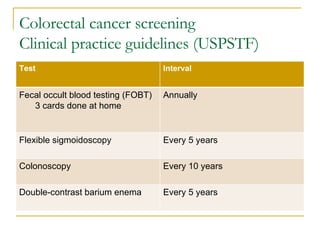
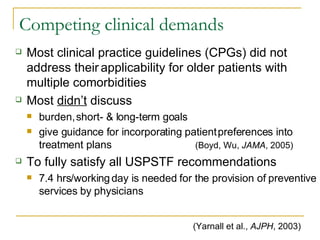
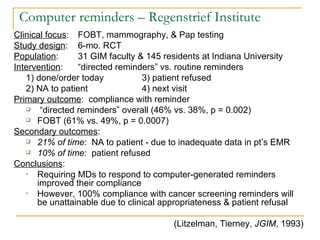
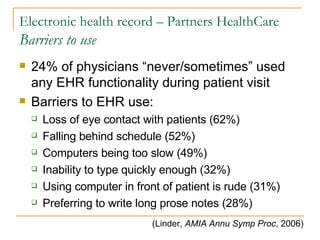


This document discusses colorectal cancer (CRC) screening guidelines and interventions to improve CRC screening rates. It outlines CRC screening tests and intervals recommended by guidelines. It also discusses competing clinical demands, barriers to electronic health records, and factors that facilitate or act as barriers to effective computer reminders and other practice interventions. Studies found that interventions incorporating computer reminders, feedback, and team-based approaches can improve CRC screening rates in practices.


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





