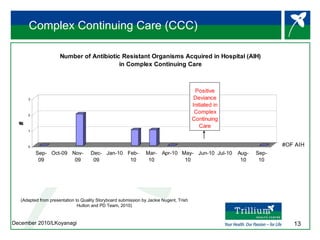
Trillium Health Centre implemented Positive Deviance methodology to reduce antibiotic resistant organisms acquired in the hospital. Key aspects of implementation included engaging frontline staff through improvisation activities to shift culture and encourage open communication. The "Nurse Jackson" concept was created to non-threateningly address infection control issues and led to staff becoming more aware of practices and collaborative in improving them. Surveys found high rates of staff knowing and using the term with positive ratings of its impact on practices. Successes are being shared more broadly and sustainability measures include ongoing audits and reporting.




























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










